

Effect of pecto-intercostal fascial block on extubation time in patients undergoing cardiac surgery: A randomized controlled trial
- PMID: 37021095
- PMCID: PMC10067611
- DOI: 10.3389/fsurg.2023.1128691
Effect of pecto-intercostal fascial block on extubation time in patients undergoing cardiac surgery: A randomized controlled trial
Abstract
Objectives: Epidural and paravertebral block reduce the extubation time in patients undergoing surgery under general anesthesia but are relatively contraindicated in heparinized patients due to the potential risk of hematoma. The Pecto-intercostal fascial block (PIFB) is an alternative in such patients.
Methods: This is a single-center randomized controlled trial. Patients scheduled for elective open cardiac surgery were randomized at a 1:1 ratio to receive PIFB (30 ml 0.3% ropivacaine plus 2.5 mg dexamethasone on each side) or saline (30 ml normal saline on each side) after induction of general anesthesia. The primary outcome was extubation time after surgery. Secondary outcomes included opioid consumption during surgery, postoperative pain scores, adverse events related to opioids, and length of stay in the hospital.
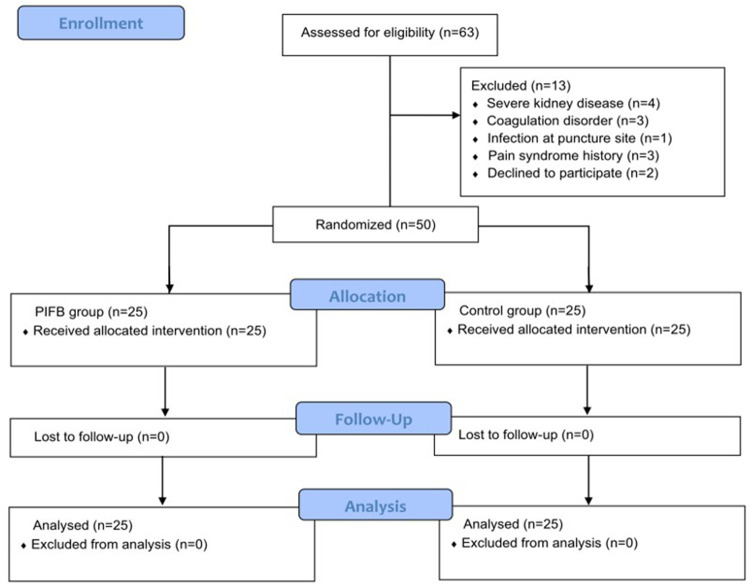
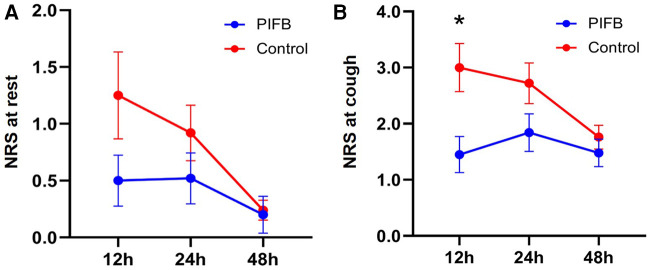
Results: A total of 50 patients (mean age: 61.8 years; 34 men) were randomized (25 in each group). The surgeries included sole coronary artery bypass grafting in 38 patients, sole valve surgery in three patients, and both procedures in the remaining nine patients. Cardiopulmonary bypass was used in 20 (40%) patients. The time to extubation was 9.4 ± 4.1 h in the PIFB group vs. 12.1 ± 4.6 h in the control group (p = 0.031). Opioid (sufentanil) consumption during surgery was 153.2 ± 48.3 and 199.4 ± 51.7 μg, respectively (p = 0.002). In comparison to the control group, the PIFB group had a lower pain score while coughing (1.45 ± 1.43 vs. 3.00 ± 1.71, p = 0.021) and a similar pain score at rest at 12 h after surgery. The two groups did not differ in the rate of adverse events.
Conclusions: PIFB decreased the time to extubation in patients undergoing cardiac surgery.
Trial registration: This trial is registered at the Chinese Clinical Trial Registry (ChiCTR2100052743) on November 4, 2021.
Keywords: analgesia; cardiac surgery; pain; pecto-intercostal fascial block; postoperative; tracheal extubation.
© 2023 Wang, Jiang, Xin, Jiang, Chen and Feng.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Effects of continuous pecto-intercostal fascial block for management of post-sternotomy pain in patients undergoing cardiac surgery: a randomized controlled trial.Int J Surg. 2025 Feb 1;111(2):2037-2045. doi: 10.1097/JS9.0000000000002200. Int J Surg. 2025. PMID: 39705137 Clinical Trial.
-
Effects of bilateral Pecto-intercostal Fascial Block for perioperative pain management in patients undergoing open cardiac surgery: a prospective randomized study.BMC Anesthesiol. 2021 Jun 22;21(1):175. doi: 10.1186/s12871-021-01391-w. BMC Anesthesiol. 2021. Retraction in: BMC Anesthesiol. 2024 Nov 29;24(1):445. doi: 10.1186/s12871-024-02839-5. PMID: 34157970 Free PMC article. Retracted. Clinical Trial.
-
Continuous Pecto-Intercostal Fascial Block Provides Effective Analgesia in Patients Undergoing Open Cardiac Surgery: A Randomized Controlled Trial.Pain Med. 2022 Mar 2;23(3):440-447. doi: 10.1093/pm/pnab291. Pain Med. 2022. PMID: 34601602 Clinical Trial.
-
Pecto-Intercostal Fascial Plane Block for Pain Management after Cardiothoracic Surgery.Curr Pain Headache Rep. 2025 May 15;29(1):84. doi: 10.1007/s11916-025-01398-9. Curr Pain Headache Rep. 2025. PMID: 40375035 Review.
-
Fast-track cardiac care for adult cardiac surgical patients.Cochrane Database Syst Rev. 2016 Sep 12;9(9):CD003587. doi: 10.1002/14651858.CD003587.pub3. Cochrane Database Syst Rev. 2016. PMID: 27616189 Free PMC article. Review.
Cited by
-
The Role of the Subcostal Transversus Abdominis Plane Block in Facilitating Operating Room Extubation After Living Donor Liver Transplantation for Hepatocellular Carcinoma: A Propensity Score-Matching Analysis.Life (Basel). 2025 Feb 14;15(2):297. doi: 10.3390/life15020297. Life (Basel). 2025. PMID: 40003706 Free PMC article.
-
Bilateral parasternal and rectus sheath blocks reduce pain post-cardiac surgery: a pilot trial.Front Surg. 2025 Feb 20;12:1526890. doi: 10.3389/fsurg.2025.1526890. eCollection 2025. Front Surg. 2025. PMID: 40052097 Free PMC article.
-
Ultrasound-Guided Analgesia in Cardiac and Breast Surgeries: A Cadaveric Comparison of SPIP Block with Single and Double Injections vs. DPIP Block.Life (Basel). 2024 Dec 31;15(1):42. doi: 10.3390/life15010042. Life (Basel). 2024. PMID: 39859982 Free PMC article.
-
Superficial Parasternal Intercostal Plane Block and Full Sternotomy; A Randomized Trial.Eur J Cardiothorac Surg. 2025 Jul 1;67(7):ezaf226. doi: 10.1093/ejcts/ezaf226. Eur J Cardiothorac Surg. 2025. PMID: 40627369 Free PMC article. Clinical Trial.
-
Impact of pecto-intercostal fascial block on postoperative fatigue in elderly patients undergoing off-pump coronary artery bypass grafting: a randomized clinical trial.Int J Surg. 2025 May 1;111(5):3323-3330. doi: 10.1097/JS9.0000000000002353. Int J Surg. 2025. PMID: 40146244 Free PMC article. Clinical Trial.
References
-
- Aydin ME, Ahiskalioglu A, Ates I, Tor IH, Borulu F, Erguney OD, et al. Efficacy of ultrasound-guided transversus thoracic muscle plane block on postoperative opioid consumption after cardiac surgery: a prospective, randomized, double-blind study. J Cardiothorac Vasc Anesth. (2020) 34:2996–3003. 10.1053/j.jvca.2020.06.044 - DOI - PubMed
LinkOut - more resources
Full Text Sources