

New Method of Tibio-calcaneal-Navicular Arthrodesis After Talectomy
- PMID: 37021118
- PMCID: PMC10068989
- DOI: 10.1177/24730114231164625
New Method of Tibio-calcaneal-Navicular Arthrodesis After Talectomy
Abstract
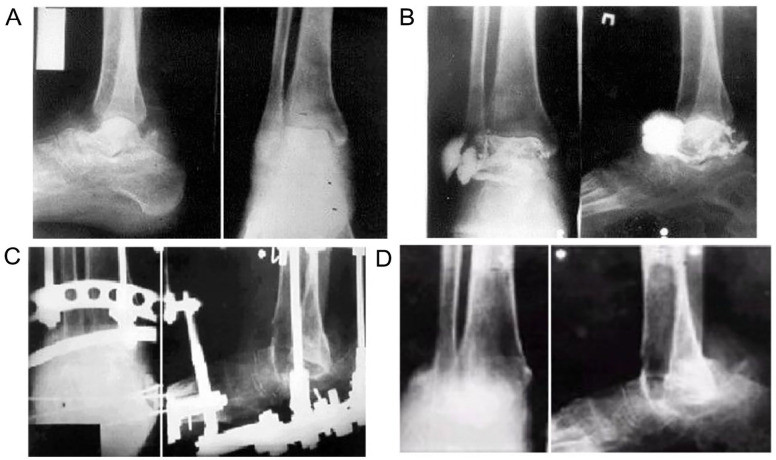
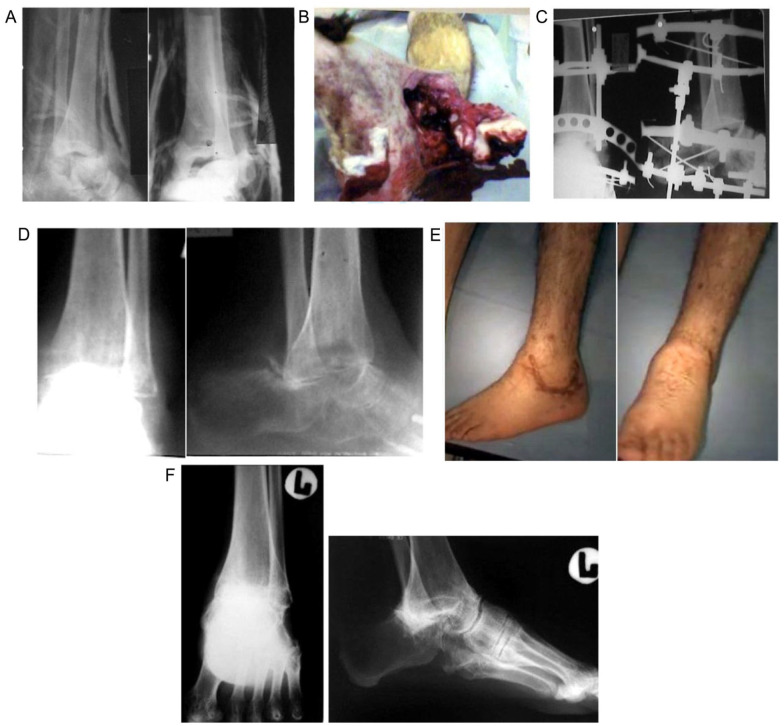
Background: After astragalectomy, patients still have a shortening of the limb, which can require various reconstructive manipulations. We have developed a simple and versatile tibio-calcaneal-navicular arthrodesis (TCNA) technique to reduce limb shortening.
Methods: The main difference from the standard method of arthrodesis between the tibia and calcaneus is that in our method after astragalectomy, the tibia rests with the anterior edge against the os navicularis, and the posterior edge against the calcaneus.We have observed 14 patients (2 were female, 12 were male) operated by a new method of tibio-calcaneal-navicular arthrodesis (TCNA) from 2003 to 2020 years with various forms of osteomyelitis, fractures, and septic necrosis of the talus. The average age of the patients was 42.2 (ranged 20-75) years. Observation results will be assessed using the American Orthopaedic Foot & Ankle Society (AOFAS) ankle-hindfoot score 1-1.5 years after surgery and treatment time in the Ilizarov apparatus.
Results: In all patients, the wounds healed by primary intention. The average time of immobilization in the apparatus was 4.9 (ranged 3.5-6) months. The average limb shortening 2.0 ± 0.5 cm. AOFAS ankle-hindfoot score (n = 14) in all patients came up to 77.9 ± 6.8 (min 68, max 86) SD 12.8. Nonunion was noted in the region of the anterior edge of the tibia in 1 patient (7.1%), and in another patient a painless nonunion was formed (7.1%). Patients wore ordinary footwear without arch supporter and with heels up to 2 cm.
Conclusion: Good and satisfactory results were obtained in all patients. The new TCNA method allows restoring the supporting ability of a limb, reduces shortening, and improves the quality of life for patients.
Level of evidence: Level IV, case series, low-quality cohort or case- control studies.
Keywords: Ilizarov apparatus; ankle joint; aseptic necrosis; astragalectomy; osteomyelitis; talus; talus fracture; tibio-calcaneal-navicular arthrodesis.
© The Author(s) 2023.
Conflict of interest statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Figures





References
-
- Canale ST, Kelly FB. Fractures of the neck of the talus. Long-term evaluation of seventy-one cases. J Bone Joint Surg Am. 1978;60(2):143-156. - PubMed
-
- Chotigavanichaya C, Ariyawatkul T, Eamsobhana P, Kaewpornsawan K. Results of primary talectomy for clubfoot in infants and toddlers with arthrogryposis multiplex congenital. J Med Assoc Thai. 2015;98(Suppl 8):38-41. - PubMed
-
- Cooper RR, Capello W. Talectomy. A long-term follow-up evaluation. Clin Orthop Relat Res. 1985;201:32-35. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials