

A dumbbell rescue stent graft facilitates clamp-free repair of aortic injury in a porcine model
- PMID: 37021144
- PMCID: PMC10068254
- DOI: 10.1016/j.jvssci.2023.100100
A dumbbell rescue stent graft facilitates clamp-free repair of aortic injury in a porcine model
Abstract
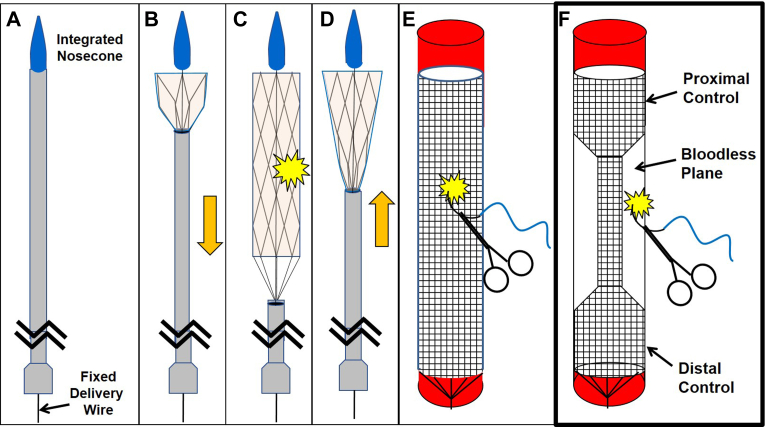
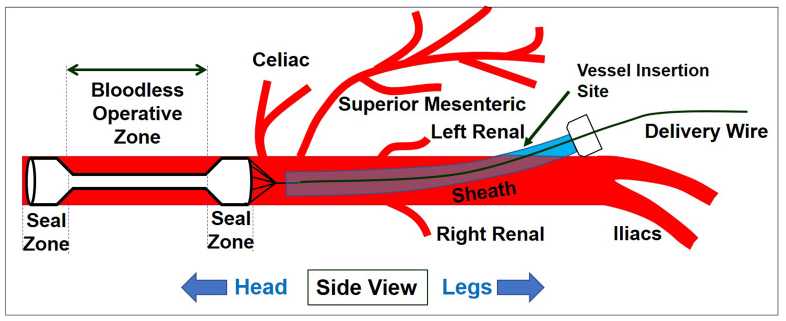
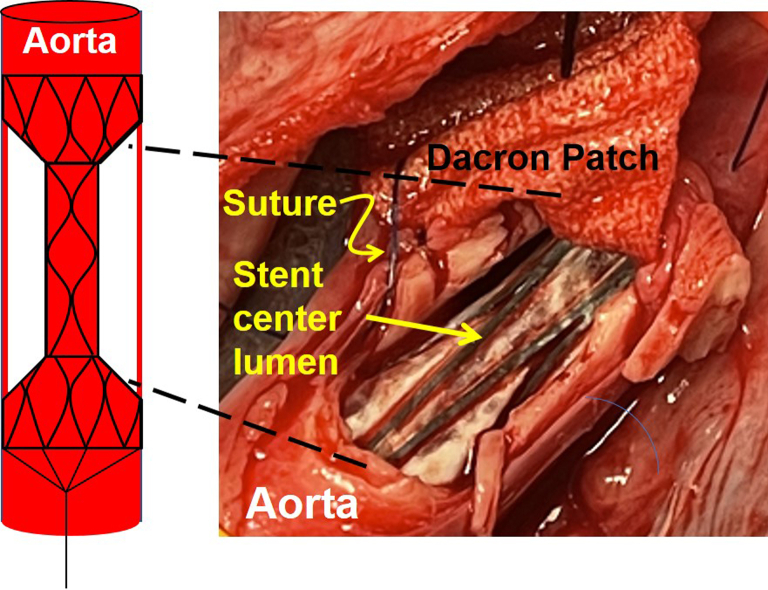
Objective: Noncompressible torso hemorrhage is a high-mortality injury. We previously reported improved outcomes with a retrievable rescue stent graft to temporize aortic hemorrhage in a porcine model while maintaining distal perfusion. A limitation was that the original cylindrical stent graft design prohibited simultaneous vascular repair, given the concern for suture ensnarement of the temporary stent. We hypothesized that a modified, dumbbell-shaped design would preserve distal perfusion and also offer a bloodless plane in the midsection, facilitating repair with the stent graft in place and improve the postrepair hemodynamics.
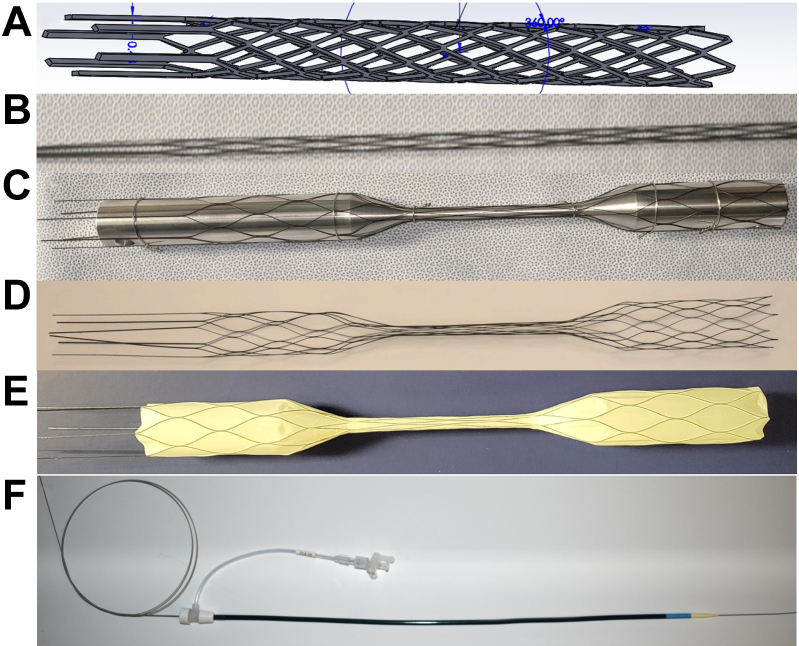
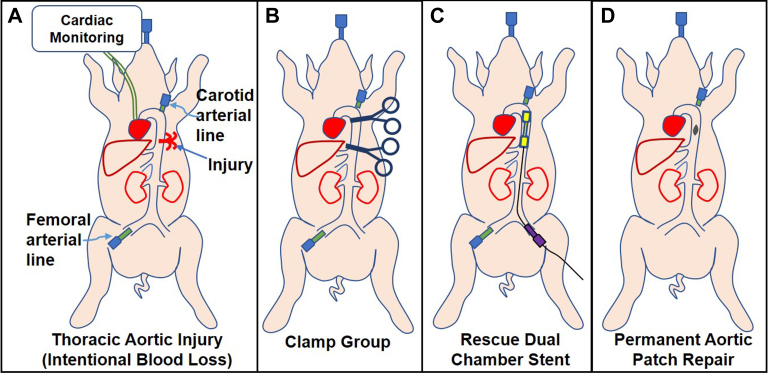
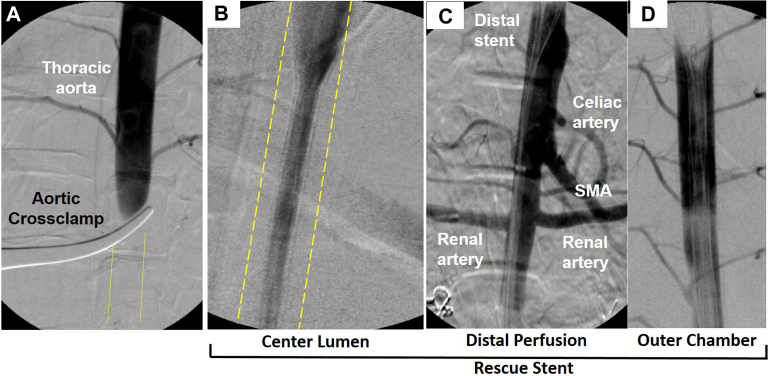
Methods: In an Institutional Animal Care and Use Committee-approved terminal porcine model, a custom retrievable dumbbell-shaped rescue stent graft (dRS) was fashioned from laser-cut nitinol and polytetrafluoroethylene covering and compared with aortic cross-clamping. Under anesthesia, the descending thoracic aorta was injured and then repaired with cross-clamping (n = 6) or dRS (n = 6). Angiography was performed in both groups. Operations were divided into phases: (1) baseline, (2) thoracic injury with either cross-clamp or dRS deployed, and (3) recovery, after which the clamp or dRS were removed. Target blood loss was 22% to simulate class II or III hemorrhagic shock. Shed blood was recovered with a Cell Saver and reinfused for resuscitation. Renal artery flow rates were recorded at baseline and during the repair phase and reported as a percentage of cardiac output. Phenylephrine pressor requirements were recorded.
Results: In contrast with cross-clamped animals, dRS animals demonstrated both operative hemostasis and preserved flow beyond the dRS angiographically. Recovery phase mean arterial pressure, cardiac output, and right ventricular end-diastolic volume were significantly higher in dRS animals (P = .033, P = .015, and P = .012, respectively). Whereas distal femoral blood pressures were absent during cross-clamping, among the dRS animals, the carotid and femoral MAPs were not significantly different during the injury phase (P = .504). Cross-clamped animals demonstrated nearly absent renal artery flow, in contrast with dRS animals, which exhibited preserved perfusion (P<.0001). Femoral oxygen levels (partial pressure of oxygen) among a subset of animals further confirmed greater distal oxygenation during dRS deployment compared with cross-clamping (P = .006). After aortic repair and clamp or stent removal, cross-clamped animals demonstrated more significant hypotension, as demonstrated by increased pressor requirements over stented animals (P = .035).
Conclusions: Compared with aortic cross-clamping, the dRS model demonstrated superior distal perfusion, while also facilitating simultaneous hemorrhage control and aortic repair. This study demonstrates a promising alternative to aortic cross-clamping to decrease distal ischemia and avoid the unfavorable hemodynamics that accompany clamp reperfusion. Future studies will assess differences in ischemic injury and physiological outcomes.
Clinical relevance: Noncompressible aortic hemorrhage remains a high-mortality injury, and current damage control options are limited by ischemic complications. We have previously reported a retrievable stent graft to allow rapid hemorrhage control, preserved distal perfusion, and removal at the primary repair. The prior cylindrical stent graft was limited by the inability to suture the aorta over the stent graft owing to risk of ensnarement. This large animal study explored a dumbbell retrievable stent with a bloodless plane to allow suture placement with the stent in place. This approach improved distal perfusion and hemodynamics over clamp repair and heralds the potential for aortic repair while avoiding complications.
Keywords: Aortic cross-clamp; Aortic trauma; Endovascular; Temporary stent; Torso hemorrhage.
Copyright © 2023 by the Society for Vascular Surgery. Published by Elsevier Inc.
Figures
Similar articles
-
A porcine model of thoracic aortic aneurysms created with a retrievable drug infusion stent graft mirrors human aneurysm pathophysiology.JVS Vasc Sci. 2024 Jul 2;5:100212. doi: 10.1016/j.jvssci.2024.100212. eCollection 2024. JVS Vasc Sci. 2024. PMID: 39188992 Free PMC article.
-
A three-tier Rescue stent improves outcomes over balloon occlusion in a porcine model of noncompressible hemorrhage.J Trauma Acute Care Surg. 2020 Aug;89(2):320-328. doi: 10.1097/TA.0000000000002715. J Trauma Acute Care Surg. 2020. PMID: 32740640 Free PMC article.
-
Damage control of caval injuries in a porcine model using a retrievable Rescue stent.J Vasc Surg Venous Lymphat Disord. 2018 Sep;6(5):646-656. doi: 10.1016/j.jvsv.2018.04.011. J Vasc Surg Venous Lymphat Disord. 2018. PMID: 30119820 Free PMC article.
-
Endovascular stent grafting and open surgical replacement for chronic thoracic aortic aneurysms: a systematic review and prospective cohort study.Health Technol Assess. 2022 Jan;26(6):1-166. doi: 10.3310/ABUT7744. Health Technol Assess. 2022. PMID: 35094747
-
Endovascular thoracic aortic repair and risk of spinal cord ischemia: the role of previous or concomitant treatment for aortic aneurysm.J Cardiovasc Surg (Torino). 2010 Apr;51(2):169-76. J Cardiovasc Surg (Torino). 2010. PMID: 20354486 Review.
Cited by
-
A porcine model of thoracic aortic aneurysms created with a retrievable drug infusion stent graft mirrors human aneurysm pathophysiology.JVS Vasc Sci. 2024 Jul 2;5:100212. doi: 10.1016/j.jvssci.2024.100212. eCollection 2024. JVS Vasc Sci. 2024. PMID: 39188992 Free PMC article.
References
-
- Morrison J.J., Rasmussen T.E. Noncompressible torso hemorrhage: a review with contemporary definitions and management strategies. Surg Clin North Am. 2012;92:843–858. vii. - PubMed
-
- Alarhayem A.Q., Myers J.G., Dent D., Liao L., Muir M., Mueller D., et al. Time is the enemy: mortality in trauma patients with hemorrhage from torso injury occurs long before the "golden hour". Am J Surg. 2016;212:1101–1105. - PubMed
-
- Brenner M., Moore L., Dubose J., Scalea T. Resuscitative endovascular balloon occlusion of the aorta (REBOA) for Use in temporizing Intra-abdominal and Pelvic hemorrhage: physiologic Sequelae and Considerations. Shock. 2020;54:615–622. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
