

Different dosing regimens of Tenecteplase in acute ischemic stroke: A network meta-analysis of the clinical evidence
- PMID: 37021171
- PMCID: PMC10069195
- DOI: 10.1177/23969873221129924
Different dosing regimens of Tenecteplase in acute ischemic stroke: A network meta-analysis of the clinical evidence
Abstract
Introduction: Acute ischemic stroke remains the major cause of death and disability and conclusive evidence of Tenecteplase in treating stroke is lacking.
Objective: To conduct a meta-analysis to determine whether Tenecteplase produces better outcomes than Alteplase and a network meta-analysis comparing the different dosing regimens of Tenecteplase.
Methods: Searches were made in MEDLINE, CENTRAL, and ClinicalTrials.gov. The outcome measures are recanalization, early neurological improvement, functional outcomes at 90 days (modified Rankin Scale 0-1 and 0-2), intracranial hemorrhage, symptomatic intracranial hemorrhage, and mortality within 90 days from treatment.
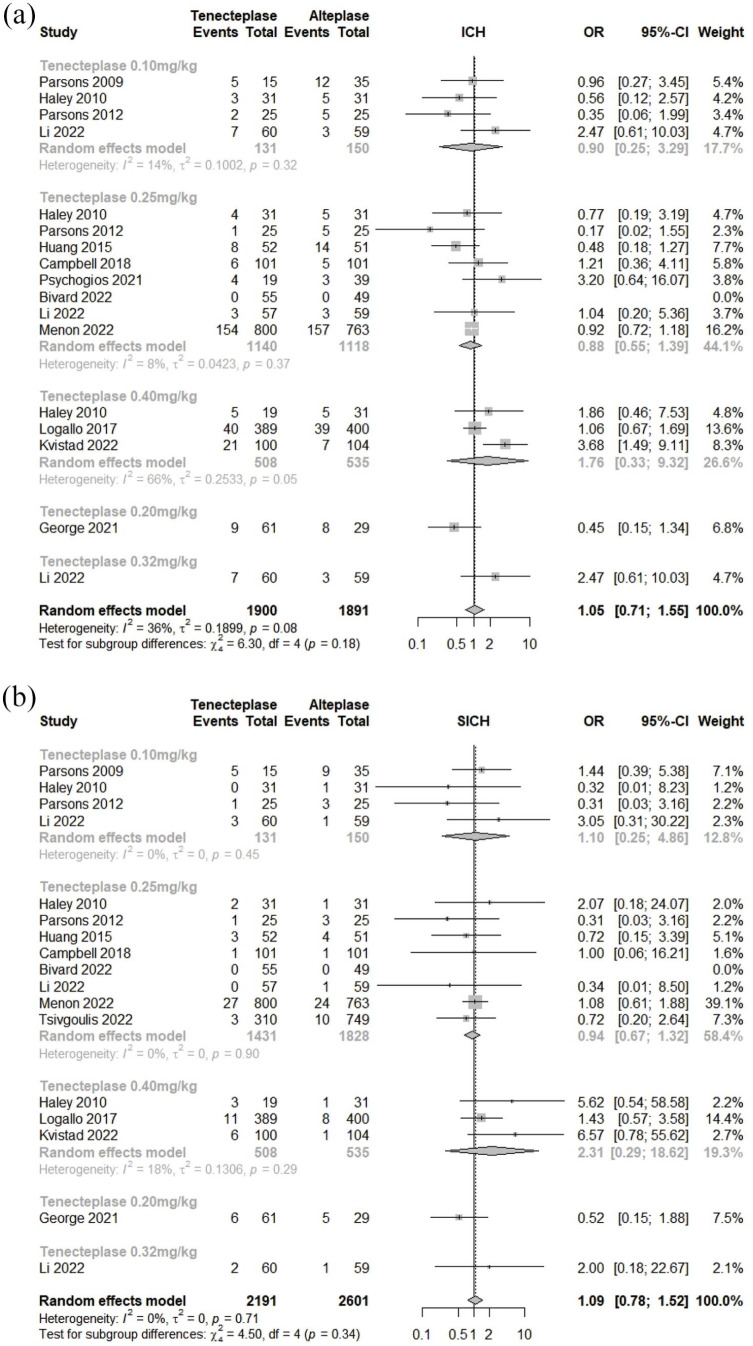
Results: Fourteen studies are included in the meta-analyses and 18 studies in the network meta-analyses. In the meta-analysis, Tenecteplase 0.25 mg/kg has significant results in early neurological improvement (OR = 2.35, and 95% CI = 1.16-4.72) and excellent functional outcome (OR = 1.20, and 95% CI = 1.02-1.42). In the network meta-analysis, Tenecteplase 0.25 mg/kg produces significant results in early neurological improvement (OR = 1.52 [95% CI = 1.13-2.05], p-value = 0.01), functional outcomes (mRS 0-1 and 0-2) (OR = 1.19 [95% CI = 1.03-1.37], p-value = 0.02; OR = 1.21 [95% CI = 1.05-1.39], p-value = 0.01; respectively) and mortality (OR = 0.78 [95% CI = 0.64-0.96], p-value = 0.02) whereas Tenecteplase 0.40 mg/kg increases the chances of symptomatic intracranial hemorrhage (OR = 2.35 [95% CI = 1.19-4.64], p-value = 0.01).
Conclusion: While not conclusive, our study lends evidence to 0.25 mg/kg Tenecteplase dose for ischemic stroke treatment. Further randomized trials need to be done to validate this finding.
Registration: International prospective register of systematic reviews (PROSPERO) - CRD42022339774URL: https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=339774.
Keywords: Alteplase; Tenecteplase; meta-analysis; network meta-analysis; stroke.
© European Stroke Organisation 2022.
Conflict of interest statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures




Similar articles
-
Complications of Intravenous Tenecteplase Versus Alteplase for the Treatment of Acute Ischemic Stroke: A Systematic Review and Meta-Analysis.Stroke. 2023 May;54(5):1192-1204. doi: 10.1161/STROKEAHA.122.042335. Epub 2023 Mar 23. Stroke. 2023. PMID: 36951049 Free PMC article.
-
Thrombolytic therapy for patients with acute ischemic stroke: systematic review and network meta-analysis of randomized trials.Front Neurol. 2025 Jan 7;15:1490476. doi: 10.3389/fneur.2024.1490476. eCollection 2024. Front Neurol. 2025. PMID: 39839875 Free PMC article.
-
Off-Label Use of Tenecteplase for the Treatment of Acute Ischemic Stroke: A Systematic Review and Meta-analysis.JAMA Netw Open. 2022 Mar 1;5(3):e224506. doi: 10.1001/jamanetworkopen.2022.4506. JAMA Netw Open. 2022. PMID: 35357458 Free PMC article.
-
Intravenous Thrombolysis With Tenecteplase in Patients With Large Vessel Occlusions: Systematic Review and Meta-Analysis.Stroke. 2021 Jan;52(1):308-312. doi: 10.1161/STROKEAHA.120.030220. Epub 2020 Dec 4. Stroke. 2021. PMID: 33272127
-
Tenecteplase Thrombolysis for Acute Ischemic Stroke.Stroke. 2020 Nov;51(11):3440-3451. doi: 10.1161/STROKEAHA.120.029749. Epub 2020 Oct 13. Stroke. 2020. PMID: 33045929 Free PMC article. Review.
Cited by
-
Protective effects of 4-HBd on blood-brain barrier integrity in MCAO/R model rats based on brain pharmacokinetic characteristics.Front Pharmacol. 2025 Apr 8;16:1528839. doi: 10.3389/fphar.2025.1528839. eCollection 2025. Front Pharmacol. 2025. PMID: 40264675 Free PMC article.
-
Tenecteplase versus alteplase for acute ischemic stroke: a systematic review and meta-analysis of randomized and non-randomized studies.J Neurol. 2024 May;271(5):2309-2323. doi: 10.1007/s00415-024-12243-1. Epub 2024 Mar 4. J Neurol. 2024. PMID: 38436679
-
Risk of intracerebral haemorrhage with tenecteplase versus alteplase in acute ischaemic stroke: a meta-analysis.J Neurol. 2025 Apr 10;272(5):334. doi: 10.1007/s00415-025-13081-5. J Neurol. 2025. PMID: 40208343 Review.
References
-
- Brown DL, Barsan WG, Lisabeth LD, et al. Survey of emergency physicians about recombinant tissue plasminogen activator for acute ischemic stroke. Ann Emerg Med 2005; 46: 56–60. - PubMed
-
- Vandelli L, Marietta M, Gambini M, et al. Fibrinogen decrease after intravenous thrombolysis in ischemic stroke patients is a risk factor for intracerebral hemorrhage. J Stroke Cerebrovasc Dis 2015; 24: 394–400. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
