

Association between type of intervention center and outcomes after endovascular treatment for acute ischemic stroke: Results from the MR CLEAN Registry
- PMID: 37021181
- PMCID: PMC10069206
- DOI: 10.1177/23969873221145771
Association between type of intervention center and outcomes after endovascular treatment for acute ischemic stroke: Results from the MR CLEAN Registry
Abstract
Background: Endovascular treatment (EVT) for acute ischemic stroke (AIS) is performed in intervention centers that provide the full range of neuro(endo)vascular care (level 1) and centers that only perform EVT for AIS (level 2). We compared outcomes between these center types and assessed whether differences in outcomes could be explained by center volume (CV).
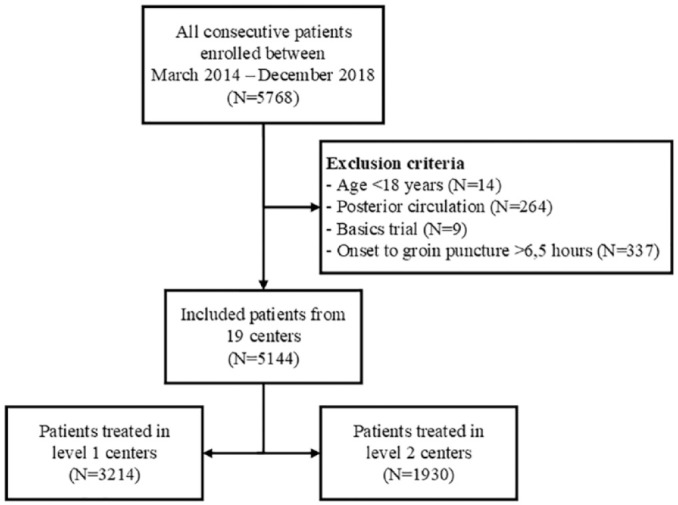
Patients and methods: We analyzed patients included in the MR CLEAN Registry (2014-2018), a registry of all EVT-treated patients in the Netherlands. Our primary outcome was the shift on the modified Rankin scale (mRS) after 90 days (ordinal regression). Secondary outcomes were the NIHSS 24-48 h post-EVT, door-to-groin time (DTGT), procedure time (linear regression), and recanalization (binary logistic regression). We compared outcomes between level 1 and 2 centers using multilevel regression models, with center as random intercept. We adjusted for relevant baseline factors, and in case of observed differences, we additionally adjusted for CV.
Results: Of the 5144 patients 62% were treated in level 1 centers. We observed no significant differences between center types in mRS (adjusted(a)cOR: 0.79, 95% CI: 0.40 to 1.54), NIHSS (aβ: 0.31, 95% CI: -0.52 to 1.14), procedure duration (aβ: 0.88, 95% CI: -5.21 to 6.97), or DTGT (aβ: 4.24, 95% CI: -7.09 to 15.57). The probability for recanalization was higher in level 1 centers compared to level 2 centers (aOR 1.60, 95% CI: 1.10 to 2.33), and this difference probably depended on CV.
Conclusions: We found no significant differences, that were independent of CV, in the outcomes of EVT for AIS between level 1 and level 2 intervention centers.
Keywords: Acute ischemic stroke; center type; endovascular treatment.
© European Stroke Organisation 2022.
Conflict of interest statement
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: DWJD reports funding from the Dutch Heart Foundation, Brain Foundation Netherlands, The Netherlands Organisation for Health Research and Development, Health Holland Top Sector Life Sciences & Health, and unrestricted grants from Penumbra Inc., Stryker, Medtronic, Thrombolytic Science, LLC, and Cerenovus for research, all paid to the institution. DWJD participated in the DSMBs of ESCAPE-NEXT (stopped July 2021) and TESLAT (without receiving payments). AAP reports an institutional grant from Siemens Healthineers & Bayer Healthcare. WHvZ received consultation fees from Stryker, Nico.Lab and Cerenovus, paid to the institution. WHvZ participates in the DSMBs of Philips’WeTrust study, Anaconda’s Solonda study, in Extremis Studies, Montpellier, all funding was paid to the institution. YBWEMR reports being a minor share-holder of Nico-Lab, not related to the current work.
References
-
- Gupta R, Horev A, Nguyen T, et al.. Higher volume endovascular stroke centers have faster times to treatment, higher reperfusion rates and higher rates of good clinical outcomes. J Neurointerv Surg 2013; 5: 294–297. - PubMed
-
- van Swieten JC, Koudstaal PJ, Visser MC, et al.. Interobserver agreement for the assessment of handicap in stroke patients. Stroke 1988; 19: 604–607. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
