

Molecular basis and therapeutic targets in prostate cancer: A comprehensive review
- PMID: 37021836
- PMCID: PMC10494850
- DOI: 10.17305/bb.2023.8782
Molecular basis and therapeutic targets in prostate cancer: A comprehensive review
Abstract
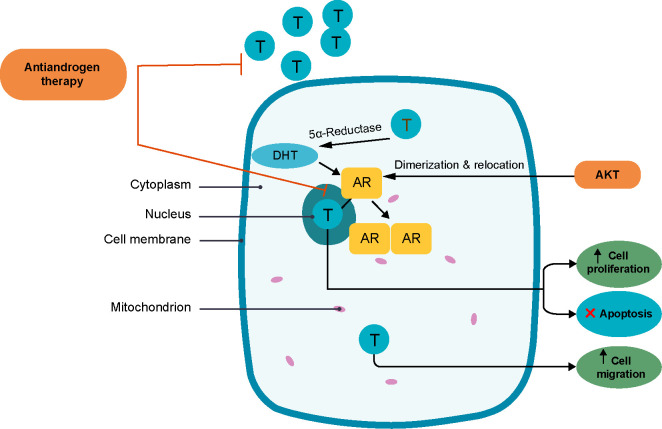
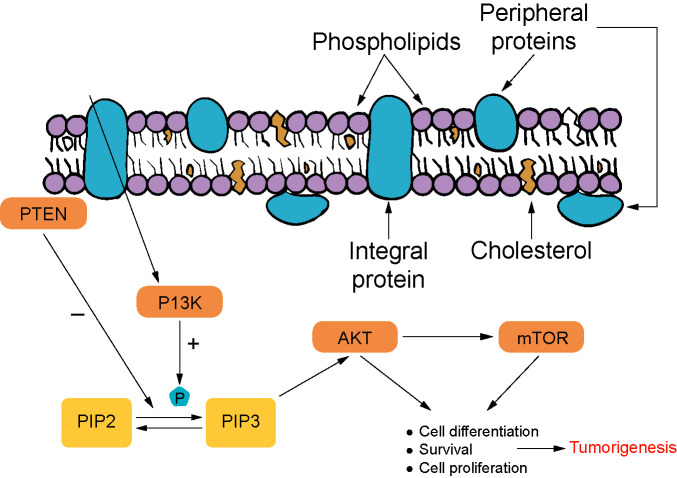
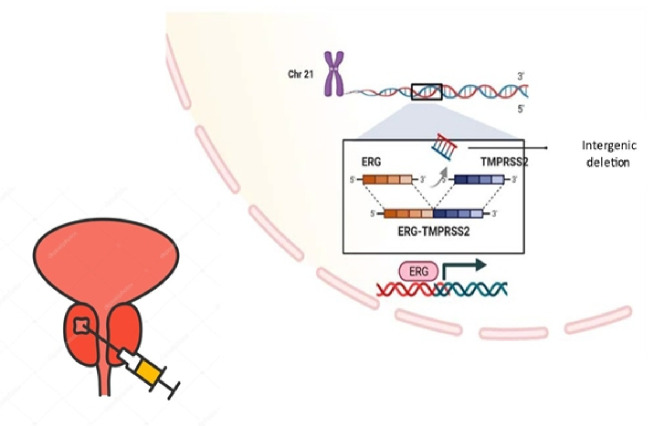
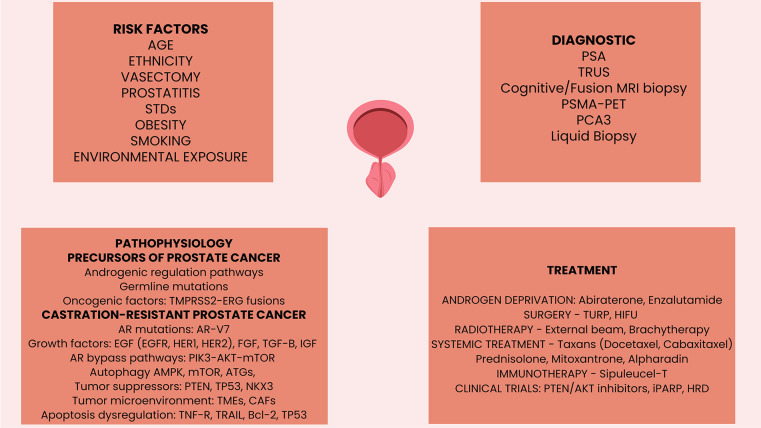
Prostate cancer is one of the most significant causes of morbidity and mortality in male patients. The incidence increases with age, and it is higher among African Americans. The occurrence of prostate cancer is associated with many risk factors, including genetic and hereditary predisposition. The most common genetic syndromes associated with prostate cancer risk are BRCA-associated hereditary breast and ovarian cancer (HBOC) and Lynch syndrome. Local-regional therapy, i.e., surgery is beneficial in early-stage prostate cancer management. Advanced and metastatic prostate cancers require systemic therapies, including hormonal inhibition, chemotherapy, and targeted agents. Most prostate cancers can be treated by targeting the androgen-receptor pathway and decreasing androgen production or binding to androgen receptors (AR). Castration-resistant prostate cancer (CRPC) usually involves the PI3K/AKT/mTOR pathway and requires targeted therapy. Specific molecular therapy can target mutated cell lines in which DNA defect repair is altered, caused by mutations of BRCA2, partner and localizer of BRCA2 (PALB2), and phosphatase and tensin homolog (PTEN) or the transmembrane protease serine 2-ERG (TMPRSS2-ERG) fusion. Most benefits were demonstrated in cyclin dependent-kinase 12 (CDK12) mutated cell lines when treated with anti-programmed cell death protein 1 (PD1) therapy. Therapies targeting p53 and AKT are the subject of ongoing clinical trials. Many genetic defects are listed as diagnostic, prognostic, and clinically actionable markers in prostate cancer. Androgen receptor splice variant 7 (AR-V7) is an important oncogenic driver and an early diagnostic and prognostic marker, as well as a therapeutic target in hormone-resistant CRPC. This review summarizes the pathophysiological mechanisms and available targeted therapies for prostate cancer.
Conflict of interest statement
Conflicts of interest: Authors declare no conflicts of interest.
Figures
References
-
- Cancer today [Internet]. Gco.iarc.fr. 2022 [cited 2022 Sep 16]. Available from: https://gco.iarc.fr/today/online-analysis.
-
- Rawla P. Epidemiology of prostate cancer. World J Oncol. 2019;10(2):63–89. https://doi.org/10.14740/wjon1191. - PMC - PubMed
-
- Merriel SWD, Funston G, Hamilton W. Prostate cancer in primary care. Adv Therapy. 2018;35(9):1285–94. https://doi.org/10.1007/s12325-018-0766-1. - PMC - PubMed
-
- Rao M. Genetic testing for prostate cancer patients. Med Clin Sci. 2020;2(1):1–2. https://doi.org/10.33425/2690-5191.1013.
-
- Çeker G, Çalışkan S. The risk factors of upgrading in prostate cancer. Cancer. 2020;126(19):4432–2. https://doi.org/10.1002/cncr.33087. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
