

Disparities in Adult Patient Selection for Extracorporeal Membrane Oxygenation in the United States: A Population-Level Study
- PMID: 37021958
- PMCID: PMC10405618
- DOI: 10.1513/AnnalsATS.202212-1029OC
Disparities in Adult Patient Selection for Extracorporeal Membrane Oxygenation in the United States: A Population-Level Study
Abstract
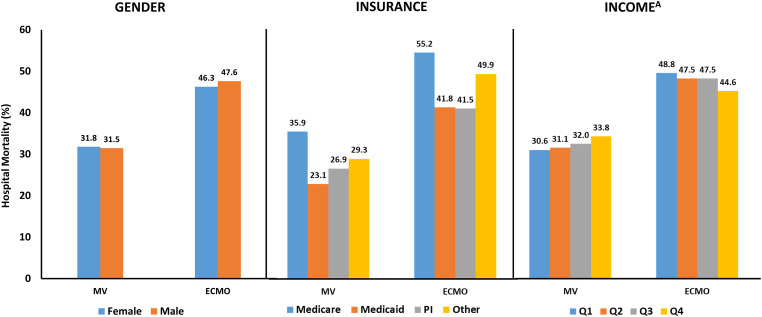
Rationale: Disparities in patient selection for advanced therapeutics in health care have been identified in multiple studies, but it is unclear if disparities exist in patient selection for extracorporeal membrane oxygenation (ECMO), a rapidly expanding critical care resource. Objectives: To determine if disparities exist in patient selection for ECMO based on sex, primary insurance, and median income of the patient's neighborhood. Methods: In a retrospective cohort study using the Nationwide Readmissions Database 2016-2019, we identified patients treated with mechanical ventilation (MV) and/or ECMO with billing codes. Patient sex, insurance, and income level for patients receiving ECMO were compared with the patients treated with MV only, and hierarchical logistic regression with the hospital as a random intercept was used to determine odds of receiving ECMO based on patient demographics. Results: We identified 2,170,752 MV hospitalizations with 18,725 cases of ECMO. Among patients treated with ECMO, 36.1% were female compared with 44.5% of patients treated with> MV only (adjusted odds ratio [aOR] for ECMO, 0.73; 95% confidence interval [CI], 0.70-0.75). Of patients treated with ECMO, 38.1% had private insurance compared with 17.4% of patients treated with MV only. Patients with Medicaid were less likely to receive ECMO than patients with private insurance (aOR, 0.55; 95% CI, 0.52-0.57). Patients treated with ECMO were more likely to live in the highest-income neighborhoods compared with patients treated with MV only (25.1% vs. 17.3%). Patients living in the lowest-income neighborhoods were less likely to receive ECMO than those living in the highest-income neighborhoods (aOR, 0.63; 95% CI, 0.60-0.67). Conclusions: Significant disparities exist in patient selection for ECMO. Female patients, patients with Medicaid, and patients living in the lowest-income neighborhoods are less likely to be treated with ECMO. Despite possible unmeasured confounding, these findings were robust to multiple sensitivity analyses. On the basis of previous work describing disparities in other areas of health care, we speculate that limited access in some neighborhoods, restrictive/biased interhospital transfer practices, differences in patient preferences, and implicit provider bias may contribute to the observed differences. Future studies with more granular data are needed to identify and modify drivers of observed disparities.
Keywords: artificial respiration; implicit bias; mechanical ventilators.
Figures
Comment in
-
Sociodemographic Disparities in Extracorporeal Membrane Oxygenation Use: Shedding Light on Codified Systemic Biases.Ann Am Thorac Soc. 2023 Aug;20(8):1105-1106. doi: 10.1513/AnnalsATS.202304-291ED. Ann Am Thorac Soc. 2023. PMID: 37526481 Free PMC article. No abstract available.
References
-
- Peek GJ, Mugford M, Tiruvoipati R, Wilson A, Allen E, Thalanany MM, et al. CESAR trial collaboration Efficacy and economic assessment of conventional ventilatory support versus extracorporeal membrane oxygenation for severe adult respiratory failure (CESAR): a multicentre randomised controlled trial. Lancet . 2009;374:1351–1363. - PubMed
-
- Combes A, Hajage D, Capellier G, Demoule A, Lavoué S, Guervilly C, et al. EOLIA Trial Group, REVA, and ECMONet Extracorporeal membrane oxygenation for severe acute respiratory distress syndrome. N Engl J Med . 2018;378:1965–1975. - PubMed
-
- Stentz MJ, Kelley ME, Jabaley CS, O’Reilly-Shah V, Groff RF, Moll V, et al. Trends in extracorporeal membrane oxygenation growth in the United States, 2011-2014. ASAIO J . 2019;65:712–717. - PubMed
-
- Thiagarajan RR, Barbaro RP, Rycus PT, Mcmullan DM, Conrad SA, Fortenberry JD, et al. ELSO member centers Extracorporeal Life Support Organization registry international report 2016. ASAIO J . 2017;63:60–67. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
