

Clinical Efficacy and Safety of a Novel Antifungal, Fosmanogepix, in Patients with Candidemia Caused by Candida auris : Results from a Phase 2 Trial
- PMID: 37022196
- PMCID: PMC10190264
- DOI: 10.1128/aac.01419-22
Clinical Efficacy and Safety of a Novel Antifungal, Fosmanogepix, in Patients with Candidemia Caused by Candida auris : Results from a Phase 2 Trial
Abstract
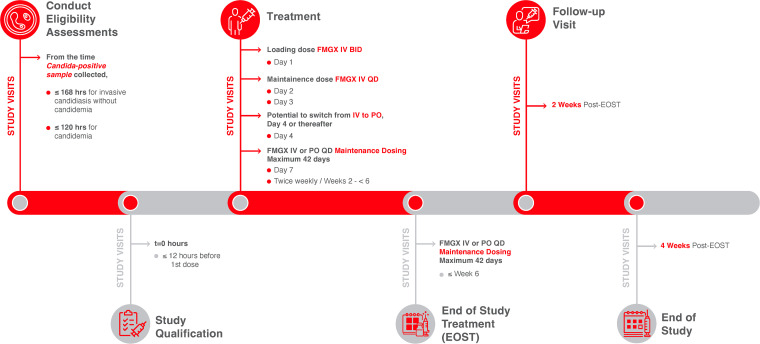
Fosmanogepix (FMGX), a novel antifungal available in intravenous (IV) and oral formulations, has broad-spectrum activity against pathogenic yeasts and molds, including fungi resistant to standard of care antifungals. This multicenter, open-label, single-arm study evaluated FMGX safety and efficacy for treatment of candidemia and/or invasive candidiasis caused by Candida auris. Eligible participants were ≥18 years, with established candidemia and/or invasive candidiasis caused by C. auris, (cultured within 120 h [for candidemia] or 168 h [for invasive candidiasis without candidemia] with accompanying clinical signs) and limited treatment options. Participants were treated with FMGX (≤42 days; loading dose: 1000 mg IV twice daily [Day 1], followed by 600 mg IV once daily [QD]). Switching to oral FMGX 800 mg QD was permitted from Day 4. Primary endpoint was treatment success (survival and clearance of C. auris from blood/tissue cultures without additional antifungals) at the end of the study treatment (EOST), assessed by an independent data review committee (DRC). Day 30 survival was a secondary endpoint. In vitro susceptibility of Candida isolates was assessed. Nine participants with candidemia (male:6, female:3; 21 to 76 years) in intensive care units in South Africa were enrolled; all received IV FMGX only. DRC-assessed treatment success at EOST and Day 30 survival were 89% (8/9). No treatment related adverse events or study drug discontinuations were reported. FMGX demonstrated potent in vitro activity against all C. auris isolates (MIC range: 0.008 to 0.015 μg/mL [CLSI]; 0.004-0.03 μg/mL [EUCAST]), with the lowest MICs compared to other antifungals tested. Thus, the results showed that FMGX was safe, well-tolerated, and efficacious in participants with candidemia caused by C. auris.
Keywords: APX001; Candida auris; Gwt1 inhibitor; candidemia; fosmanogepix; intensive care unit.
Conflict of interest statement
The authors declare a conflict of interest. Jose A. Vazquez received grant support from Cidara, Scynexis and was a consultant for Cidara, Scynexis, F2G, Amplyx. Michael R. Hodges, Eric Ople, Pamela Wedel were employees of Amplyx (now a Pfizer Inc subsidiary). Michael R. Hodges was previously an employee of Pfizer and holds Pfizer stock. Paul A. Bien and Margaret Tawadrous are employees of Pfizer and hold Pfizer stock. Iwona Oborska was a consultant for Amplyx, previously a Pfizer employee, and Pfizer shareholder. Fathima Paruk has served on the speaker bureaus for Thermofischer Scientific, Pfizer, Biomerieux, MSD and Dr Reddy's. Peter G. Pappas received grant support from Astellas, Gilead, Mayne, Cidara, Scynexis and provided advisory and consultancy services to Amplyx, Mayne, Scynexis. Kenneth Boffard has no conflicts of interest to declare.
Figures
References
-
- Chow NA, Muñoz JF, Gade L, Berkow EL, Li X, Welsh RM, Forsberg K, Lockhart SR, Adam R, Alanio A, Alastruey-Izquierdo A, Althawadi S, Araúz AB, Ben-Ami R, Bharat A, Calvo B, Desnos-Ollivier M, Escandón P, Gardam D, Gunturu R, Heath CH, Kurzai O, Martin R, Litvintseva AP, Cuomo CA. 2020. Tracing the evolutionary history and global expansion of Candida auris using population genomic analyses. mBio 11:e03364-19. doi:10.1128/mBio.03364-19. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
