

Haemorrhage-related maternal mortality in Bangladesh: Levels, trends, time of death, and care-seeking practices based on nationally representative population-based surveys
- PMID: 37022713
- PMCID: PMC10080499
- DOI: 10.7189/jogh.13.07001
Haemorrhage-related maternal mortality in Bangladesh: Levels, trends, time of death, and care-seeking practices based on nationally representative population-based surveys
Abstract
Background: Haemorrhage is a major cause of maternal deaths globally, most of which are preventable and predominantly happen in low and middle-income countries, including Bangladesh. We examine the current levels, trends, time of death, and care-seeking practices for haemorrhage-related maternal deaths in Bangladesh.
Methods: We conducted a secondary analysis with data from the nationally representative 2001, 2010, and 2016 Bangladesh Maternal Mortality Surveys (BMMS). The cause of death information was collected through verbal autopsy (VA) interviews using a country-adapted version of the standard World Health Organization VA questionnaire. Trained physicians reviewed the VA questionnaire and assigned the cause of death using the International Classification of Diseases (ICD) codes.
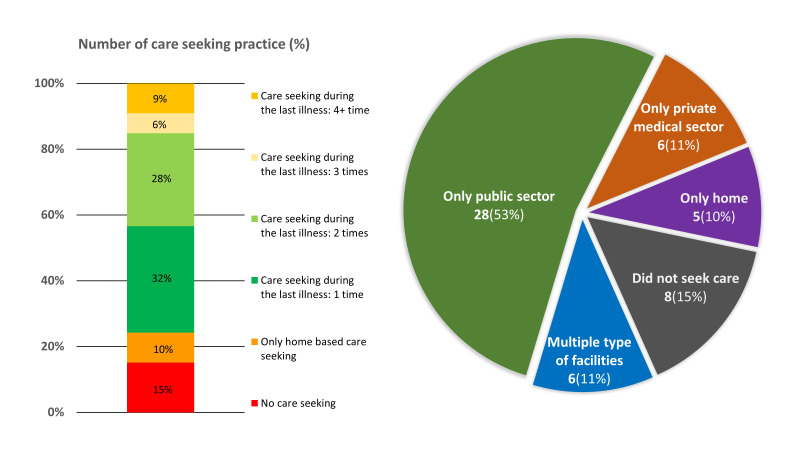
Results: Haemorrhage accounted for 31% (95% confidence interval (CI) = 24-38) of all maternal deaths in 2016 BMMS, which was 31% (95% CI = 25-41) in 2010 BMMS and 29% (95% CI = 23-36) in 2001 BMMS. The haemorrhage-specific mortality rate remained unchanged between 2010 BMMS (60 per 100 000 live births, uncertainty range (UR) = 37-82) and 2016 BMMS (53 per 100 000 live births, UR = 36-71). Around 70% of haemorrhage-related maternal deaths took place within 24 hours of delivery. Of those who died, 24% did not seek health care outside the home and 15% sought care from more than three places. Approximately two-thirds of the mothers who died due to haemorrhage gave birth at home.
Conclusions: Postpartum haemorrhage remains the primary cause of maternal mortality in Bangladesh. To reduce these preventable deaths, the Government of Bangladesh and stakeholders should take steps to ensure community awareness about care-seeking during delivery.
Copyright © 2023 by the Journal of Global Health. All rights reserved.
Conflict of interest statement
Disclosure of interest: The authors completed the ICMJE Disclosure of Interest Form (available upon request from the corresponding authors) and disclose no relevant interest.
Figures







Similar articles
-
Preeclampsia and eclampsia-specific maternal mortality in Bangladesh: Levels, trends, timing, and care-seeking practices.J Glob Health. 2023 Jul 14;13:07003. doi: 10.7189/jogh.13.07003. J Glob Health. 2023. PMID: 37441775 Free PMC article.
-
Levels, trends, causes, place and time of, care-seeking for, and barriers in preventing indirect maternal deaths in Bangladesh: An analysis of national-level household surveys.J Glob Health. 2023 Apr 28;13:04019. doi: 10.7189/jogh.13.04019. J Glob Health. 2023. PMID: 37114719 Free PMC article.
-
Levels and trends in mortality and causes of death among women of reproductive age in Bangladesh: Findings from three national surveys.J Glob Health. 2023 Aug 25;13:07005. doi: 10.7189/jogh.13.07005. J Glob Health. 2023. PMID: 37616128 Free PMC article.
-
Child mortality in Bangladesh - why, when, where and how? A national survey-based analysis.J Glob Health. 2021 Sep 11;11:04052. doi: 10.7189/jogh.11.04052. eCollection 2021. J Glob Health. 2021. PMID: 34552721 Free PMC article.
-
Underreporting and misclassification of maternal mortality in Taiwan.Acta Obstet Gynecol Scand. 1997 Aug;76(7):629-36. doi: 10.3109/00016349709024602. Acta Obstet Gynecol Scand. 1997. PMID: 9292636 Review.
Cited by
-
Healthcare-Seeking Behaviour for Obstetric Complications in Ethiopia: A Multilevel Mixed-Effect Analysis.Health Serv Insights. 2025 Jun 24;18:11786329251347353. doi: 10.1177/11786329251347353. eCollection 2025. Health Serv Insights. 2025. PMID: 40567355 Free PMC article.
-
Midwives' experiences with implementation of active management of third stage of labor in Sub-Saharan Africa: a systematic review.BMC Pregnancy Childbirth. 2025 May 8;25(1):547. doi: 10.1186/s12884-025-07331-7. BMC Pregnancy Childbirth. 2025. PMID: 40340625 Free PMC article.
-
Preeclampsia and eclampsia-specific maternal mortality in Bangladesh: Levels, trends, timing, and care-seeking practices.J Glob Health. 2023 Jul 14;13:07003. doi: 10.7189/jogh.13.07003. J Glob Health. 2023. PMID: 37441775 Free PMC article.
-
A context-driven approach through stakeholder engagement to introduce a digital emergency obstetric and newborn care register into routine obstetric health care services in Bangladesh.J Glob Health. 2024 May 10;14:04098. doi: 10.7189/jogh.14.04098. J Glob Health. 2024. PMID: 38721686 Free PMC article.
-
Introducing a digital emergency obstetric and newborn care register for indoor obstetric patient management: An implementation research in selected public health care facilities of Bangladesh.J Glob Health. 2024 May 10;14:04075. doi: 10.7189/jogh.14.04075. J Glob Health. 2024. PMID: 38722093 Free PMC article.
References
-
- Royal College of Obstetricians & Gynaecologists. Antepartum Haemorrhage, Green-top Guideline No.63. Available: https://www.rcog.org.uk/media/pwdi1tef/gtg_63.pdf. Accessed: 18 January 2023.
-
- GBD 2015 Disease and Injury Incidence and Prevalence Collaborators Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990–2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet. 2016;388:1545-602. 10.1016/S0140-6736(16)31678-6 - DOI - PMC - PubMed
-
- World Health Organization. WHO recommendations for the prevention and treatment of postpartum haemorrhage 2012. Available: https://apps.who.int/iris/bitstream/handle/10665/75411/9789241548502_eng.... Accessed: 18 January 2023. - PubMed
-
- Dolea C, AbouZahr C. Global burden of maternal haemorrhage in the year 2000. Geneva: World Health Organization; 2003.
