

How does obesity affect mortality through blood pressure and blood glucose in Chinese and US citizens? Insights from a causal mediation analysis of two large cohorts
- PMID: 37022778
- PMCID: PMC10078858
- DOI: 10.7189/jogh.13.04032
How does obesity affect mortality through blood pressure and blood glucose in Chinese and US citizens? Insights from a causal mediation analysis of two large cohorts
Abstract
Background: Obesity, which has reached the scale of a global pandemic, is a leading cause of premature death. It is unclear to what extent its effect on mortality was driven by blood pressure or glucose levels in people of different ethnicities.
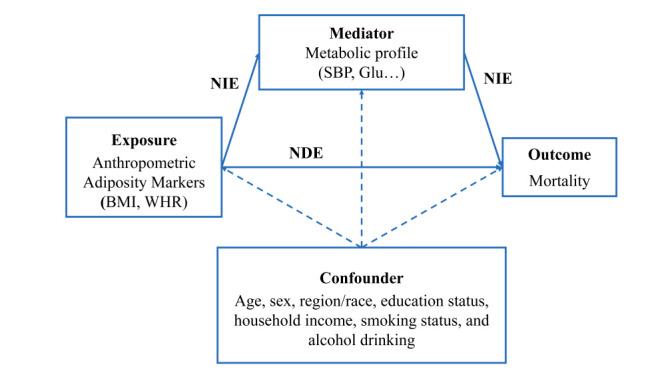
Methods: We conducted a causal mediation analysis to estimate the mediation effect of blood pressure and glucose between body mass index (BMI) or waist-hip ratio (WHR) on mortality based on data from the China Kadoorie Biobank (CKB) (n = 458 385) and US National Health and Nutrition Examination Survey (NHANES) (1999-2008, n = 20 726).
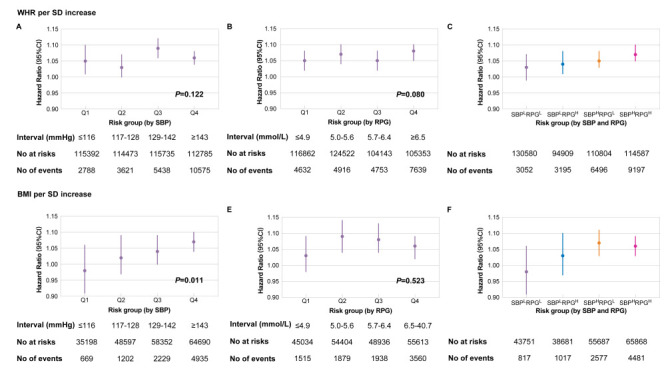
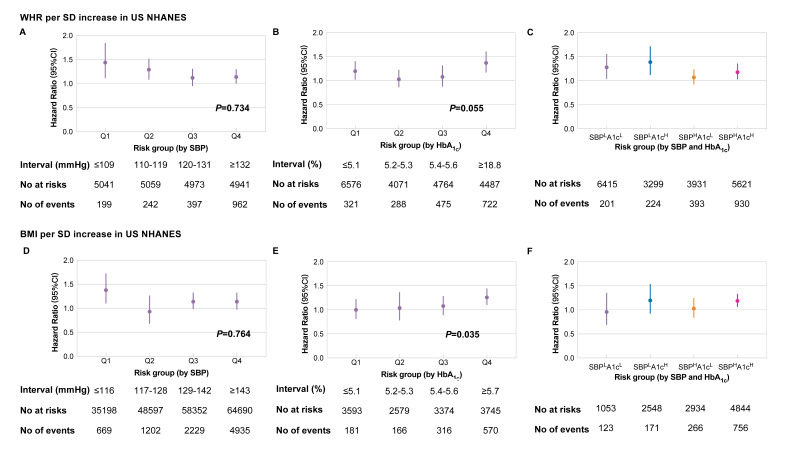
Results: The WHR's effect on mortality was mediated by blood pressure and glucose in the CKB data set by 38.7% (95% confidence interval (CI) = 34.1, 43.2) and 36.4% (95% CI = 31.6, 42.8), whereas in NHANES by 6.0% (95% CI = 2.3, 8.3) and 11.2% (95% CI = 4.7, 22.7), respectively. For associations between BMI and mortality in subjects with overweight or obesity, the mediator proportion of blood glucose and pressure was 49.4% (95% CI = 40.1, 62.5) and 16.9% (95% CI = 13.6, 22.9) in CKB and 9.10% (95% CI = 2.2, 25.9) and 16.7% (95% CI = 7.3, 49.0) in NHANES, respectively. We stratified the patients by their blood glucose, blood pressure level, or both into four groups. The effect of WHR on mortality was comparable across subgroups in either cohort. The associations between BMI and mortality were stronger in patients with higher blood pressure in CKB (P = 0.011) and blood glucose in NHANES (P = 0.035) in patients with overweight and obesity.
Conclusions: The relationship between WHR and mortality in the CKB data set was potentially caused by blood pressure and glucose to a much greater extent than in the NHANES one. The effect of BMI influenced by blood pressure was significantly higher among Chinese individuals with overweight and obesity. These results implicate a different intervention strategy is required for blood pressure and blood glucose in China and US to prevent obesity and obesity-related premature death.
Copyright © 2023 by the Journal of Global Health. All rights reserved.
Conflict of interest statement
Disclosure of interest: The authors completed the ICMJE Disclosure of Interest Form (available upon request from the corresponding author) and disclose no relevant interests.
Figures
References
-
- NCD Risk Factor Collaboration (NCD-RisC) Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: a pooled analysis of 2416 population-based measurement studies in 128.9 million children, adolescents, and adults. Lancet. 2017;390:2627-42. 10.1016/S0140-6736(17)32129-3 - DOI - PMC - PubMed
-
- Bogers RP, Bemelmans WJ, Hoogenveen RT, Boshuizen HC, Woodward M, Knekt P, et al. Association of overweight with increased risk of coronary heart disease partly independent of blood pressure and cholesterol levels: a meta-analysis of 21 cohort studies including more than 300 000 persons. Arch Intern Med. 2007;167:1720-8. 10.1001/archinte.167.16.1720 - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
