

A Healthy Diet is Associated with a Lower Risk of Hepatic Fibrosis
- PMID: 37023964
- PMCID: PMC10273161
- DOI: 10.1016/j.tjnut.2023.03.038
A Healthy Diet is Associated with a Lower Risk of Hepatic Fibrosis
Abstract
Background: Higher diet quality is associated with a lower risk of NAFLD.
Objectives: We examined the relationship between diet quality and hepatic fibrosis.
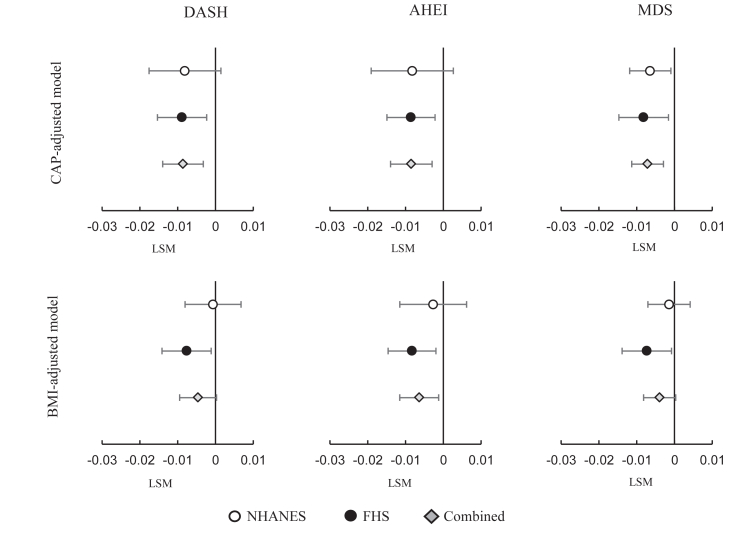
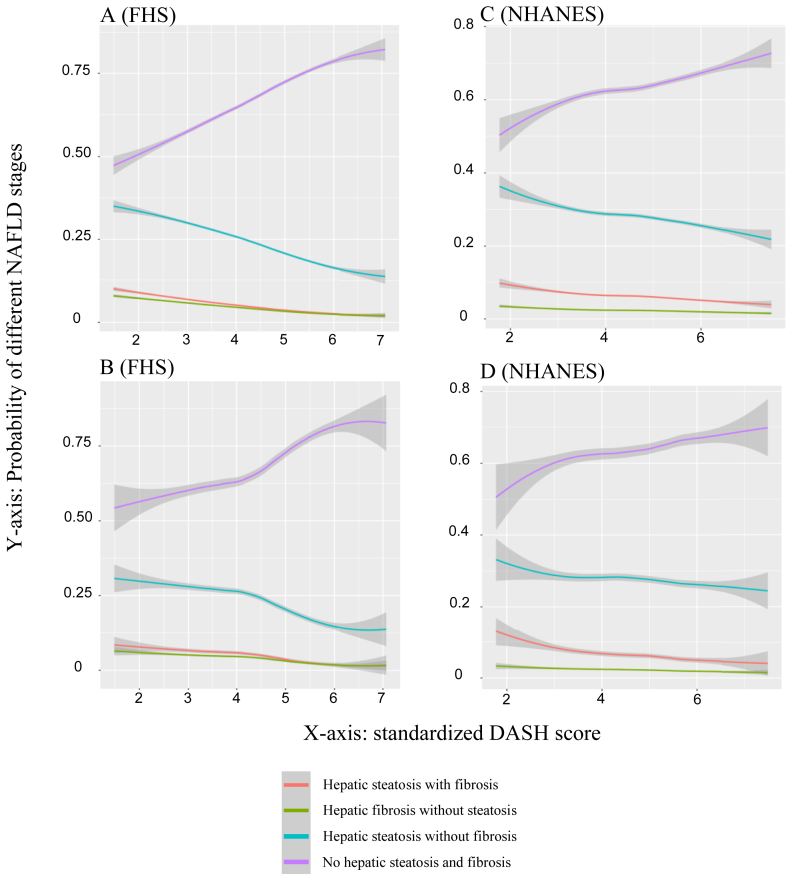
Methods: We analyzed cross-sectional associations between 3 a priori diet quality scores-the Dietary Approaches to Stop Hypertension (DASH) score, the Alternative Healthy Eating Index (AHEI), and a modified Mediterranean-style Diet Score (MDS)-and hepatic fat [controlled attenuation parameter (CAP)] and fibrosis [liver stiffness measurement (LSM)] measured by vibration-controlled transient elastography (VCTE) in 2532 Framingham Heart Study (FHS) participants and 3295 participants of the National Health and Nutrition Examination Survey (NHANES).
Results: Higher diet quality scores were associated with lower LSM in both FHS and NHANES after adjustment for demographic and lifestyle factors. Additional adjustment for CAP or BMI attenuated the observed associations. Association strength was similar across all 3 diet quality scores. Fixed-effect meta-analysis demonstrated that, under CAP-adjusted models, the LSM decreases associated with 1-SD increase of the DASH, AHEI, and MDS scores were 2% (95% CI: 0.7%, 3.3%; P = 0.002), 2% (95% CI: 0.7%, 3.3%; P = 0.003), and 1.7% (95% CI: 0.7%, 2.6%; P = 0.001), respectively, whereas in the meta-analysis of BMI-adjusted models, LSM reductions associated with 1-SD increase of the DASH, AHEI, and MDS scores were 2.2% (95% CI: -0.1%, 2.2%; P = 0.07), 1.5% (95% CI: 0.3%, 2.7%; P = 0.02), and 0.9 (95% CI: -0.1%, 1.9%; P = 0.07), respectively.
Conclusions: We demonstrated associations of higher diet quality with favorable hepatic fat and fibrosis measures. Our data suggest that a healthy diet may reduce the likelihood of obesity and hepatic steatosis as well as the progression of steatosis to fibrosis.
Keywords: DASH score; Framingham Heart Study; NHANES; hepatic fat; hepatic fibrosis; liver fat; nonalcoholic fatty liver disease; vibration-controlled transient elastography.
Copyright © 2023 American Society for Nutrition. All rights reserved.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
