

Wnt7a deficit is associated with dysfunctional angiogenesis in pulmonary arterial hypertension
- PMID: 37024132
- PMCID: PMC10259331
- DOI: 10.1183/13993003.01625-2022
Wnt7a deficit is associated with dysfunctional angiogenesis in pulmonary arterial hypertension
Abstract
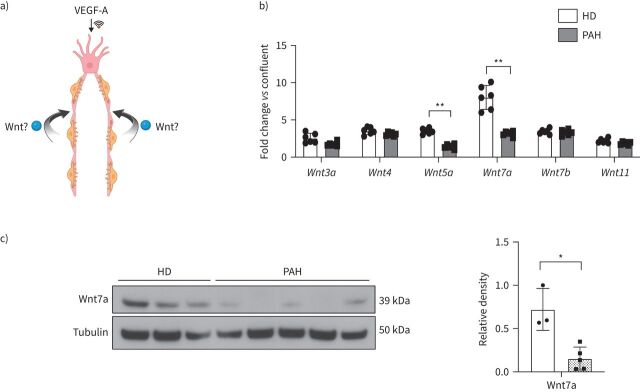
Introduction: Pulmonary arterial hypertension (PAH) is characterised by loss of microvessels. The Wnt pathways control pulmonary angiogenesis but their role in PAH is incompletely understood. We hypothesised that Wnt activation in pulmonary microvascular endothelial cells (PMVECs) is required for pulmonary angiogenesis, and its loss contributes to PAH.
Methods: Lung tissue and PMVECs from healthy and PAH patients were screened for Wnt production. Global and endothelial-specific Wnt7a -/- mice were generated and exposed to chronic hypoxia and Sugen-hypoxia (SuHx).
Results: Healthy PMVECs demonstrated >6-fold Wnt7a expression during angiogenesis that was absent in PAH PMVECs and lungs. Wnt7a expression correlated with the formation of tip cells, a migratory endothelial phenotype critical for angiogenesis. PAH PMVECs demonstrated reduced vascular endothelial growth factor (VEGF)-induced tip cell formation as evidenced by reduced filopodia formation and motility, which was partially rescued by recombinant Wnt7a. We discovered that Wnt7a promotes VEGF signalling by facilitating Y1175 tyrosine phosphorylation in vascular endothelial growth factor receptor 2 (VEGFR2) through receptor tyrosine kinase-like orphan receptor 2 (ROR2), a Wnt-specific receptor. We found that ROR2 knockdown mimics Wnt7a insufficiency and prevents recovery of tip cell formation with Wnt7a stimulation. While there was no difference between wild-type and endothelial-specific Wnt7a -/- mice under either chronic hypoxia or SuHx, global Wnt7a +/- mice in hypoxia demonstrated higher pulmonary pressures and severe right ventricular and lung vascular remodelling. Similar to PAH, Wnt7a +/- PMVECs exhibited an insufficient angiogenic response to VEGF-A that improved with Wnt7a.
Conclusions: Wnt7a promotes VEGF signalling in lung PMVECs and its loss is associated with an insufficient VEGF-A angiogenic response. We propose that Wnt7a deficiency contributes to progressive small vessel loss in PAH.
Copyright ©The authors 2023.
Conflict of interest statement
Conflict of interest: V.A. de Jesus Perez reports support for the present manuscript from the National Institutes of Health National Heart, Lung, and Blood Institute; and outside the submitted work, holds a leadership position as AHA Chair of Diversity subcommittee. All other authors have nothing to disclose.
Figures














Comment in
-
Too hot? Too cold? Wnt signalling in pulmonary arterial hypertension: can we treat it "just right"?Eur Respir J. 2023 Jun 8;61(6):2300504. doi: 10.1183/13993003.00504-2023. Print 2023 Jun. Eur Respir J. 2023. PMID: 37290809 No abstract available.
References
-
- Galiè N, Humbert M, Vachiery JL, et al. . 2015 ESC/ERS guidelines for the diagnosis and treatment of pulmonary hypertension. Rev Esp Cardiol 2016: 69: 177. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous