

The epifascial cap: A typical imaging sign for subcutaneous granuloma annulare in children
- PMID: 37025295
- PMCID: PMC10071042
- DOI: 10.3389/fped.2023.1069428
The epifascial cap: A typical imaging sign for subcutaneous granuloma annulare in children
Abstract
Objectives: Subcutaneous granuloma annulare (SGA) is a rare, self-limiting granulomatous disease in children, commonly diagnosed by histopathology following biopsy or surgical excision. This study aimed to identify imaging clues for SGA that could expedite accurate diagnosis and avoid the need for biopsy in children.
Methods: We retrospectively analyzed complete hospital records of all children diagnosed with SGA at our institution from January 2001 to December 2020. Detailed disease history, imaging findings, management, and outcome were evaluated.
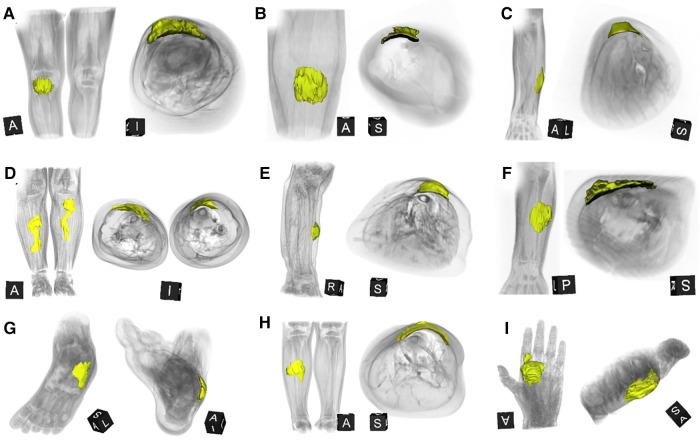
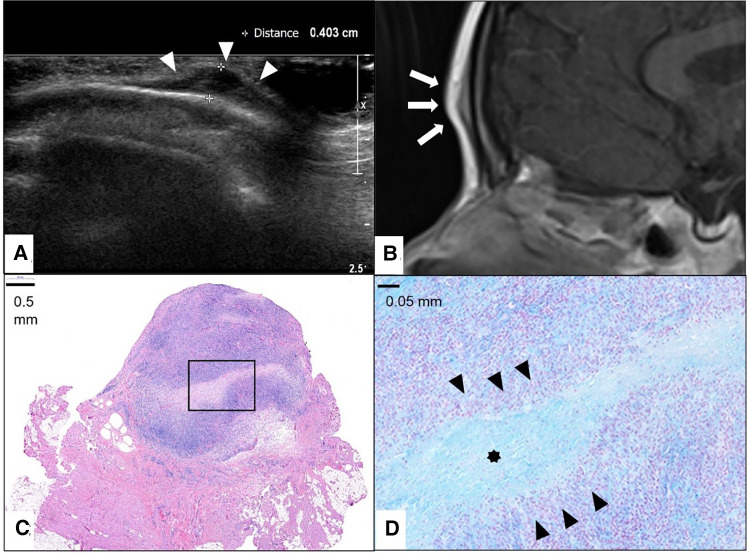
Results: We identified 28 patients (20 girls) at a median age of 3.75 (range 1-12.5 years). Ten patients presented with multiple lesions. Most lesions were located on the lower extremities (n = 26/41). Ultrasound examinations were performed on all patients, and 12 (43%) patients also received an MRI. Surgical intervention was conducted in 18 (64%) patients either by incisional biopsy (n = 6) or total excision of the lump (n = 12). In all patients who did not undergo surgery, SGA resolved spontaneously. A careful review of the MRIs led to the discovery of a characteristic imaging shape of SGA lesions: the epifascial cap with a typical broad circular base laying on the fascia, extending towards the subdermal/dermal tissue. This distinctive shape was evident in every patient in our cohort.
Conclusions: The "Epifascial Cap Sign" is a specific imaging sign for SGA, which to the best of our knowledge, helps distinguish this disease from other subcutaneous lesions. Recognition of this novel diagnostic sign combined with the historical and physical findings should enable clinicians to establish SGA diagnosis easily and diminish the need for further invasive diagnostic procedures.
Keywords: benign lesion; children; granuloma annulare; lumps and bumps; self limiting disease; subcutaneous lesion; treatment.
© 2023 Beqo, Tschauner, Gasparella, Brcic and Haxhija.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures





Similar articles
-
Subcutaneous Granuloma Annulare vs. Subcutaneous Vascular Malformations in Children: A Diagnostic Challenge.Children (Basel). 2023 Feb 11;10(2):362. doi: 10.3390/children10020362. Children (Basel). 2023. PMID: 36832491 Free PMC article.
-
Subcutaneous Granuloma Annulare.Acta Dermatovenerol Croat. 2017 Dec;25(4):292-294. Acta Dermatovenerol Croat. 2017. PMID: 30064602
-
Subcutaneous granuloma annulare: a systematic review of a rare and underdiagnosed disease.Int J Dermatol. 2025 Feb;64(2):246-255. doi: 10.1111/ijd.17419. Epub 2024 Aug 1. Int J Dermatol. 2025. PMID: 39090834
-
Surgical management and outcome of scalp subcutaneous granuloma annulare in children: case report.Neurosurgery. 2008 Nov;63(5):E1002; discussion E1002. doi: 10.1227/01.NEU.0000333264.11514.FE. Neurosurgery. 2008. PMID: 19005364
-
Subcutaneous granuloma annulare: MR imaging features in six children and literature review.Radiology. 1999 Mar;210(3):845-9. doi: 10.1148/radiology.210.3.r99mr11845. Radiology. 1999. PMID: 10207490 Review.
References
-
- Patrizi A, Gurioli C, Neri I. Childhood granuloma annulare: a review. G Ital Dermatol Venereol. (2014) 149:663–74. PMID: . - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous