

Hypertensive posterior reversible encephalopathy causing obstructive hydrocephalus
- PMID: 37025546
- PMCID: PMC10070290
- DOI: 10.25259/SNI_963_2022
Hypertensive posterior reversible encephalopathy causing obstructive hydrocephalus
Abstract
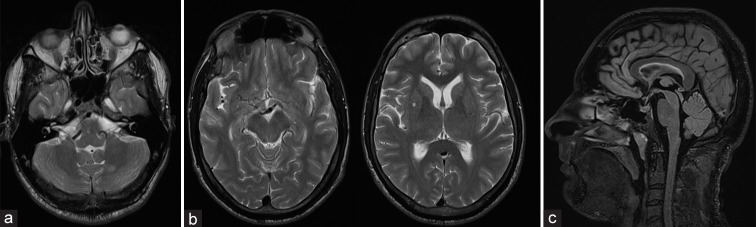
Background: Posterior reversible encephalopathy syndrome (PRES) can occur due to the detrimental effect of malignant hypertension on cerebral autoregulation. Most reported cases describe involvement of the supratentorial areas. Involvement of the posterior fossa structures in conjunction with supratentorial involvement has also been reported; however, PRES affecting the infratentorial structures without supratentorial involvement is a rare phenomenon. Clinical manifestations can involve severe headache, seizures, and reduced consciousness with treatment focused primarily on blood pressure control.
Case description: We report a case of PRES with isolated involvement of the infratentorial structures leading to obstructive hydrocephalus. The patient was managed with aggressive control of blood pressure and avoided ventriculostomy or posterior fossa decompression with a good outcome.
Conclusion: Medical management in the absence of neurological deficit can be associated with a good outcome.
Keywords: Cerebral autoregulation; Hypertensive encephalopathy; Obstructive hydrocephalus; Posterior fossa oedema.
Copyright: © 2023 Surgical Neurology International.
Conflict of interest statement
There are no conflicts of interest.
Figures


References
-
- Abusabha Y, Petridis AK, Kraus B, Kamp MA, Steiger HJ, Beseoglu K. Life-threatening posterior reversible encephalopathy syndrome in the cerebellum treated by posterior fossa decompression. Acta Neurochir (Wien) 2017;159:1325–8. - PubMed
-
- Chang GY, Keane JR. Hypertensive brainstem encephalopathy: Three cases presenting with severe brainstem edema. Neurology. 1999;53:652–4. - PubMed
-
- Cruz-Flores S, de Assis Aquino Gondim F, Leira EC. Brainstem involvement in hypertensive encephalopathy: Clinical and radiological findings. Neurology. 2004;62:1417–9. - PubMed
-
- Grossbach AJ, Abel TJ, Hodis B, Wassef SN, Greenlee JD. Hypertensive posterior reversible encephalopathy syndrome causing posterior fossa edema and hydrocephalus. J Clin Neurosci. 2014;21:207–11. - PubMed
Publication types
LinkOut - more resources
Full Text Sources