

Contemporary patterns of lipoprotein(a) testing and associated clinical care and outcomes
- PMID: 37025553
- PMCID: PMC10070377
- DOI: 10.1016/j.ajpc.2023.100478
Contemporary patterns of lipoprotein(a) testing and associated clinical care and outcomes
Abstract
Objective: Elevated lipoprotein(a) [Lp(a)] is associated with atherosclerotic cardiovascular disease, yet little is known about Lp(a) testing patterns in real-world practice. The objective of this analysis was to determine how Lp(a) testing is used in clinical practice in comparison with low density lipoprotein cholesterol (LDL-C) testing alone, and to determine whether elevated Lp(a) level is associated with subsequent initiation of lipid-lowering therapy (LLT) and incident cardiovascular (CV) events.
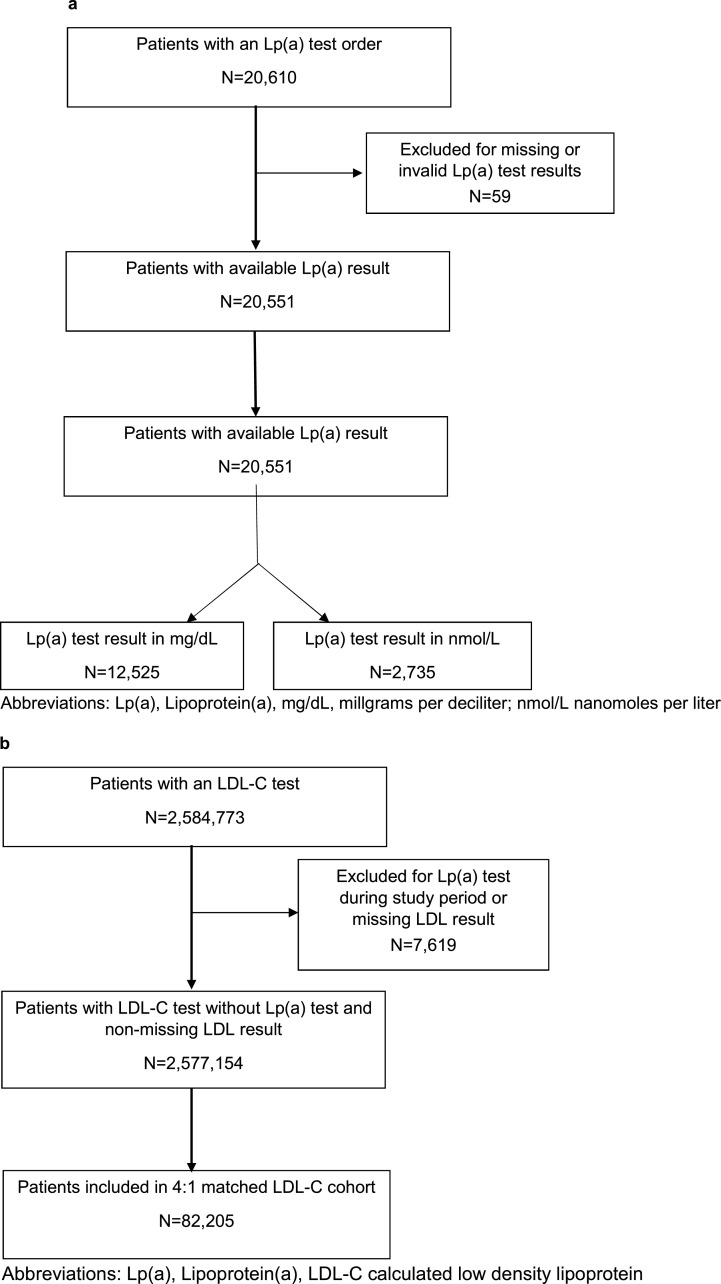
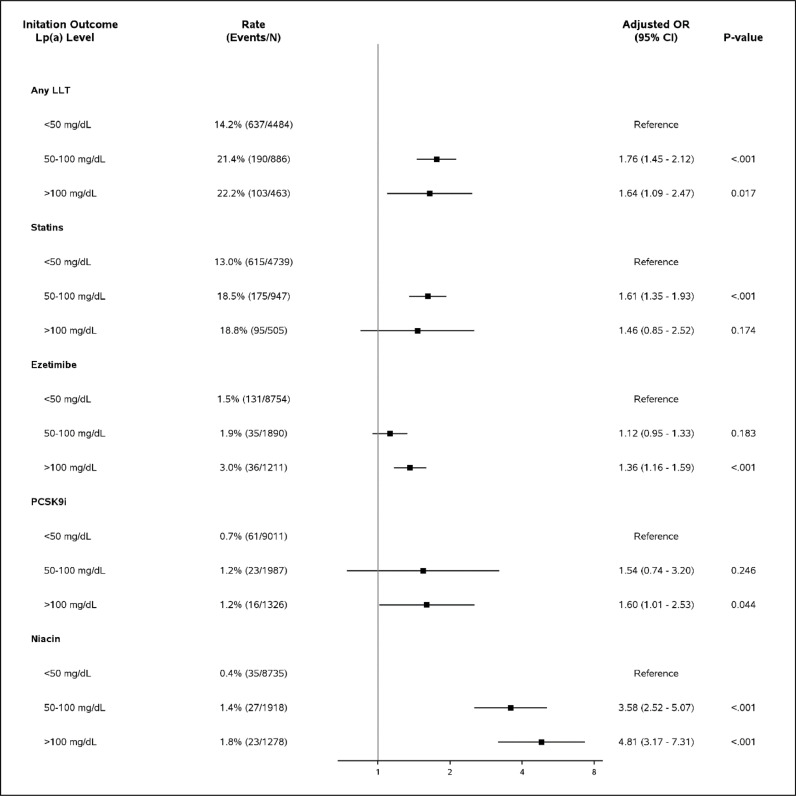
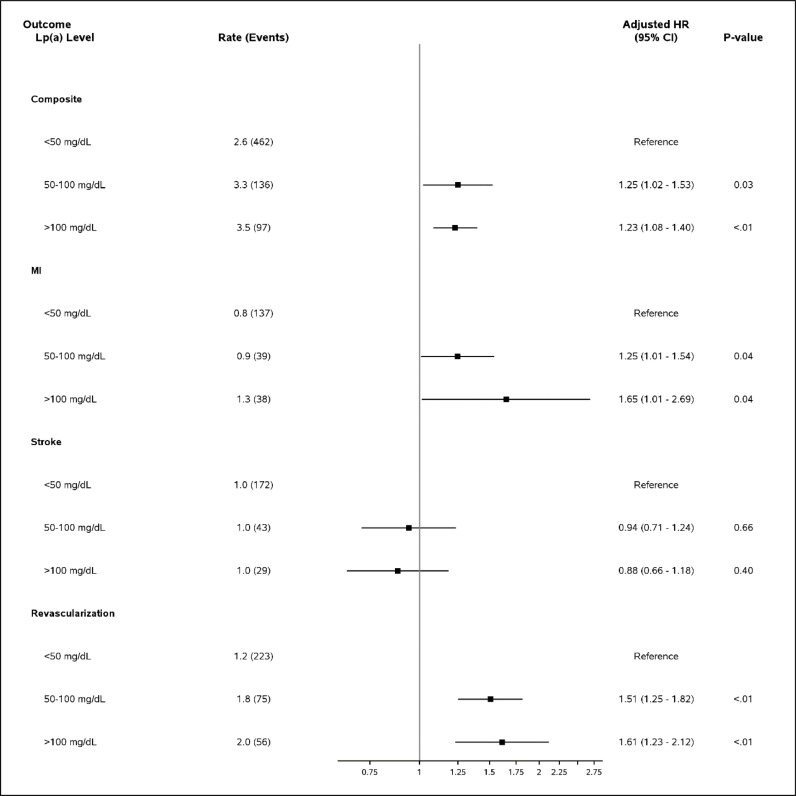
Methods: This is an observational cohort study, based on lab tests administered between Jan 1, 2015 and Dec 31, 2019. We used electronic health record (EHR) data from 11 United States health systems participating in the National Patient-Centered Clinical Research Network (PCORnet). We created two cohorts for comparison: 1) the Lp(a) cohort, of adults with an Lp(a) test and 2) the LDL-C cohort, of 4:1 date- and site-matched adults with an LDL-C test, but no Lp(a) test. The primary exposure was the presence of an Lp(a) or LDL-C test result. In the Lp(a) cohort, we used logistic regression to assess the relationship between Lp(a) results in mass units (< 50, 50-100, and > 100mg/dL) and molar units (<125, 125-250, > 250nmol/L) and initiation of LLT within 3 months. We used multivariable adjusted Cox proportional hazards regression to evaluate these Lp(a) levels and time to composite CV hospitalization, including hospitalization for myocardial infarction, revascularization and ischemic stroke.
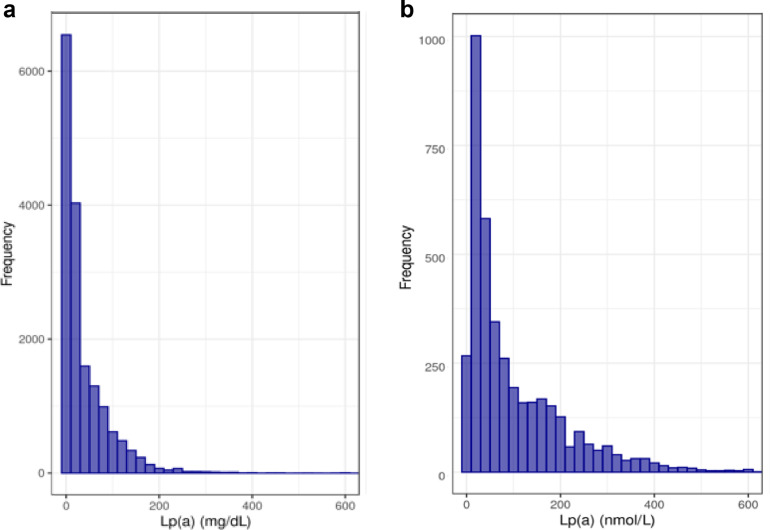
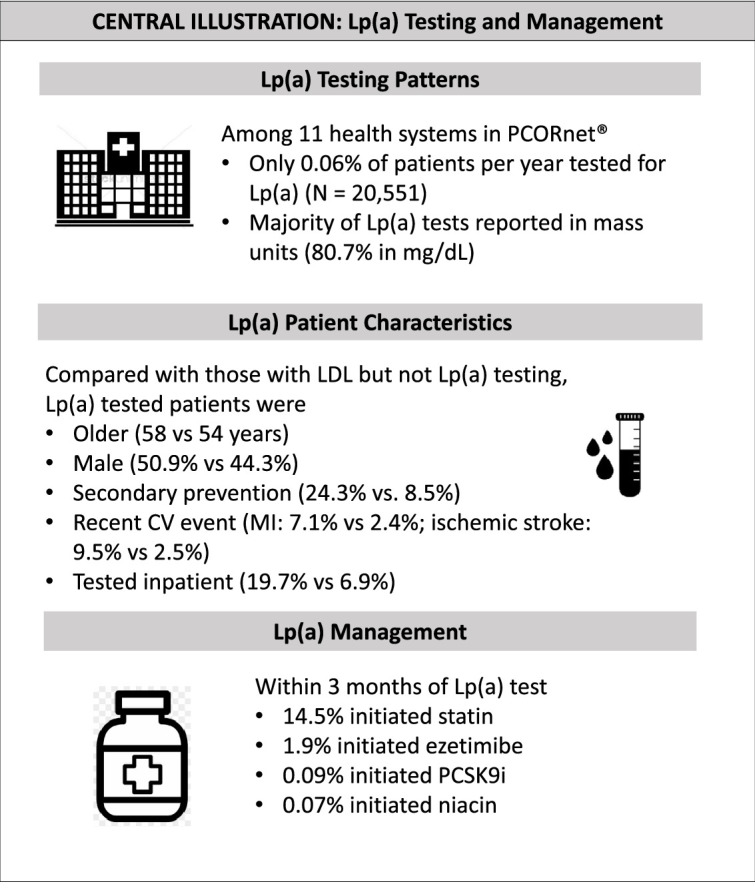
Results: Overall, 20,551 patients had Lp(a) test results and 2,584,773 patients had LDL-C test results (82,204 included in the matched LDL-C cohort). Compared with the LDL-C cohort, the Lp(a) cohort more frequently had prevalent ASCVD (24.3% vs. 8.5%) and multiple prior CV events (8.6% vs. 2.6%). Elevated Lp(a) was associated with greater odds of subsequent LLT initiation. Elevated Lp(a) reported in mass units was also associated with subsequent composite CV hospitalization [aHR (95% CI): Lp(a) 50-100mg/dL 1.25 (1.02-1.53), p<0.03, Lp(a) > 100mg/dL 1.23 (1.08-1.40), p<0.01].
Conclusion: Lp(a) testing is relatively infrequent in health systems across the U.S. As new therapies for Lp(a) emerge, improved patient and provider education is needed to increase awareness of the utility of this risk marker.
Keywords: Cardiovascular prevention; Lipoprotein(a).
©2023TheAuthors.PublishedbyElsevierB.V.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper. Michelle D Kelsey reports financial support was provided by Amgen Inc. Disclosures: PHJ reports grant support from the Make Well Known Foundation through an unrestricted grant from Amgen; grant support from Novartis and Novo Nordisk. MFL has received research funding from the NIH (HL116263), Amgen, Regeneron, Ionis, Merck, REGENXBIO, Sanofi and Novartis and has served as a consultant for Esperion, Alexion Pharmaceuticals and REGENXBIO. EDP reports research support from: Amgen Inc., Janssen Pharmaceutical Products, Bristol Myers Squibb, Esperion; and consulting fees from: Jansen Pharmaceutical Products, Boehringer Ingelheim, Novartis, Cerner. NJP reports research grants from: Amgen, Inc.; AstraZeneca; Baseline Study LLC; Boehringer Ingleheim; Duke Clinical Research Institute; Eli Lilly & Company; Novartis Pharmaceuticals, Novo Nordisk Pharmaceutical Company; Regeneron Pharmaceuticals, Inc.; Sanofi-S.A.; Verily Sciences Research Company; Consulting fees from AstraZeneca; Boehringer Ingleheim; Esperion Therapeutics, Eli Lilly & Company, Novo Nordisk Pharmaceutical Company. The remaining authors have nothing to disclose.
Figures
References
-
- Wilson DP, Jacobson TA, Jones PH, Koschinsky ML, McNeal CJ, Nordestgaard BG, et al. Use of Lipoprotein(a) in clinical practice: a biomarker whose time has come. A scientific statement from the National Lipid Association. J Clin Lipidol. 2019;13(3):374–392. - PubMed
-
- Tsimikas S. A test in context: lipoprotein(a): diagnosis, prognosis, controversies, and emerging therapies. J Am Coll Cardiol. 2017;69(6):692–711. - PubMed
-
- Welsh P, Welsh C, Celis-Morales CA, Brown R, Ho FK, Ferguson LD, et al. Lipoprotein(a) and cardiovascular disease: prediction, attributable risk fraction, and estimating benefits from novel interventions. Eur J Prevent Cardiol. 2020 - PubMed
-
- Clarke R, Peden JF, Hopewell JC, Kyriakou T, Goel A, Heath SC, et al. Genetic variants associated with Lp(a) lipoprotein level and coronary disease. N Engl J Med. 2009;361(26):2518–2528. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
