

Establishment of a nomogram model for acute chest pain triage in the chest pain center
- PMID: 37025691
- PMCID: PMC10070711
- DOI: 10.3389/fcvm.2023.930839
Establishment of a nomogram model for acute chest pain triage in the chest pain center
Abstract
Background: Acute myocardial infarction (AMI) is the leading life-threatening disease in the emergency department (ED), so rapid chest pain triage is important. This study aimed to establish a clinical prediction model for the risk stratification of acute chest pain patients based on the Point-of-care (POC) cardiac troponin (cTn) level and other clinical variables.
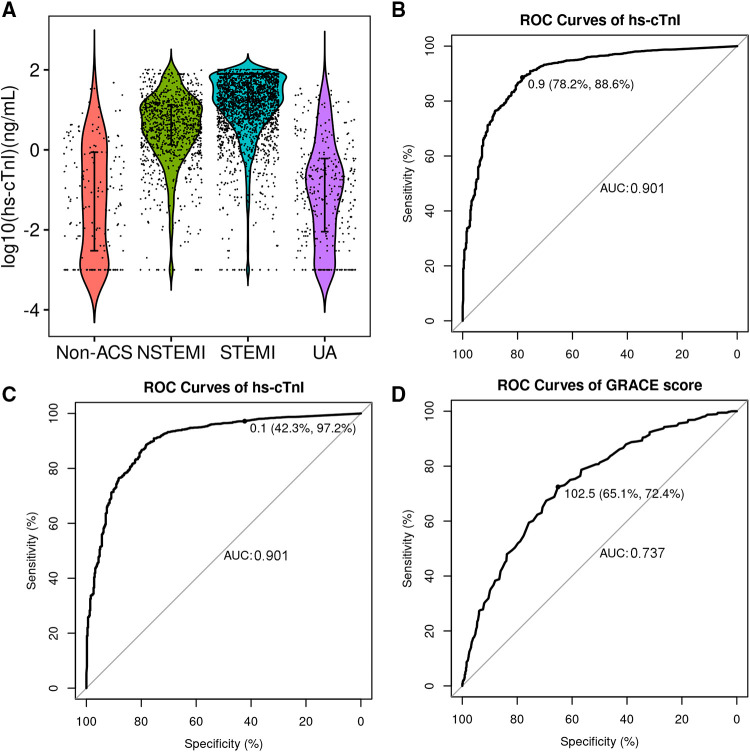
Methods: We conducted a post-hoc analysis of the database from 6,019 consecutive patients (excluding prehospital-diagnosed non-cardiac chest pain patients) attending a local chest pain center (CPC) in China between October 2016 and January 2019. The plasma concentration of cardiac troponin I (cTnI) was measured using a POC cTnI (Cardio Triage, Alere) assay. All the eligible patients were randomly divided into training and validation cohorts by a 7:3 ratio. We performed multivariable logistic regression to select variables and build a nomogram based on the significant predictive factors. We evaluated the model's generalization ability of diagnostic accuracy in the validation cohort.
Results: We analyzed data from 5,397 patients that were included in this research. The median turnaround time (TAT) of POC cTnI was 16 min. The model was constructed with 6 variables: ECG ischemia, POC cTnI level, hypotension, chest pain symptom, Killip class, and sex. The area under the ROC curve (AUC) in the training and validation cohorts was 0.924 and 0.894, respectively. The diagnostic performance was superior to the GRACE score (AUC: 0.737).
Conclusion: A practical predictive model was created and could be used for rapid and effective triage of acute chest pain patients in the CPC.
Keywords: acute chest pain triage; acute coronary syndrome; acute myocardial infarction; point-of-care (POC); troponin.
© 2023 Yan, Wei, Li and Song.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures



Similar articles
-
Point-of-Care Troponin Testing during Ambulance Transport to Detect Acute Myocardial Infarction.Prehosp Emerg Care. 2020 Nov-Dec;24(6):751-759. doi: 10.1080/10903127.2020.1721740. Epub 2020 Mar 3. Prehosp Emerg Care. 2020. PMID: 31985326
-
Evaluation of a point-of-care assay for cardiac markers for patients suspected of acute myocardial infarction.Clin Chim Acta. 2004 Aug 16;346(2):211-9. doi: 10.1016/j.cccn.2004.03.036. Clin Chim Acta. 2004. PMID: 15256323
-
Assessing sensitivity and specificity of the Manchester Triage System in the evaluation of acute coronary syndrome in adult patients in emergency care: a systematic review protocol.JBI Database System Rev Implement Rep. 2015 Nov;13(11):64-73. doi: 10.11124/jbisrir-2015-2213. JBI Database System Rev Implement Rep. 2015. PMID: 26657465
-
Chest pain centers: diagnosis of acute coronary syndromes.Ann Emerg Med. 2000 May;35(5):449-61. Ann Emerg Med. 2000. PMID: 10783407 Review.
-
Serum markers in the emergency department diagnosis of acute myocardial infarction.Emerg Med Clin North Am. 2001 May;19(2):321-37. doi: 10.1016/s0733-8627(05)70186-3. Emerg Med Clin North Am. 2001. PMID: 11373981 Review.
References
-
- Pollack CV, Jr, Braunwald E. 2007 Update to the ACC/AHA guidelines for the management of patients with unstable angina and non-ST-segment elevation myocardial infarction: implications for emergency department practice. Ann Emerg Med. (2008) 51(5):591–606. 10.1016/j.annemergmed.2007.09.004 - DOI - PubMed
-
- Desch S, Freund A, Graf T, Fichtlscherer S, Haake H, Preusch M, et al. Immediate unselected coronary angiography versus delayed triage in survivors of out-of-hospital cardiac arrest without ST-segment elevation: design and rationale of the TOMAHAWK trial. Am Heart J. (2019) 209:20–8. 10.1016/j.ahj.2018.12.005 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials