

Low haemoglobin level predicts early hospital readmission in patients with cirrhosis and acute decompensation
- PMID: 37025944
- PMCID: PMC10070139
- DOI: 10.1016/j.jhepr.2023.100698
Low haemoglobin level predicts early hospital readmission in patients with cirrhosis and acute decompensation
Abstract
Background & aims: Patients with decompensated cirrhosis present frequent hospitalisations with a relevant clinical and socio-economic impact. This study aims to characterise unscheduled readmissions up to 1-year follow-up and identify predictors of 30-day readmission after an index hospitalisation for acute decompensation (AD).
Methods: We performed a secondary analysis of a prospectively collected cohort of patients admitted for AD. Laboratory and clinical data at admission and at discharge were collected. Timing and causes of unscheduled readmissions and mortality were recorded up to 1 year.
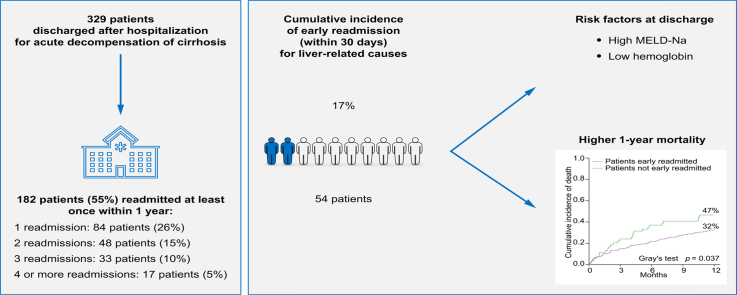
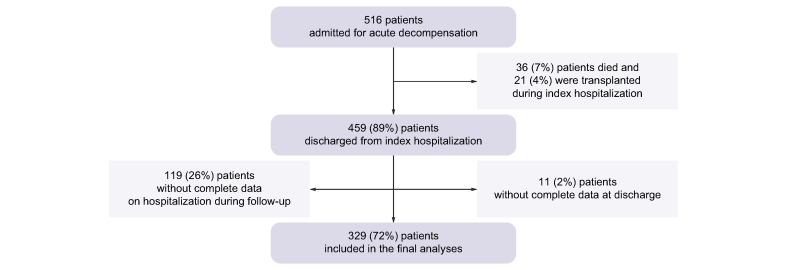
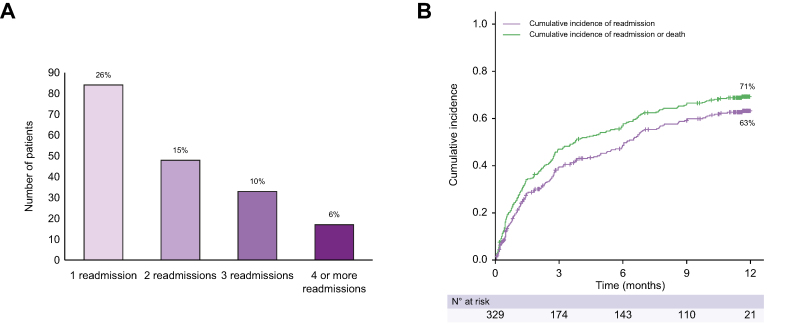
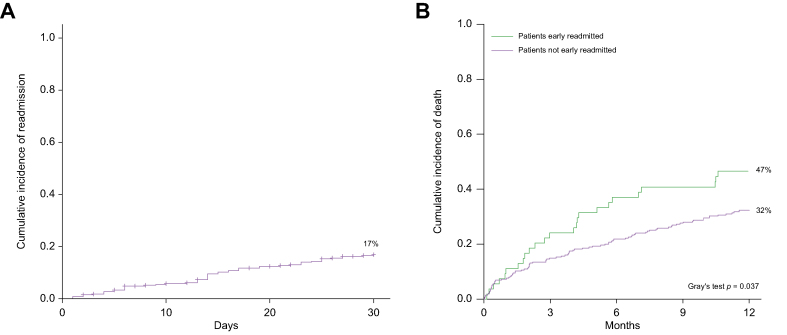
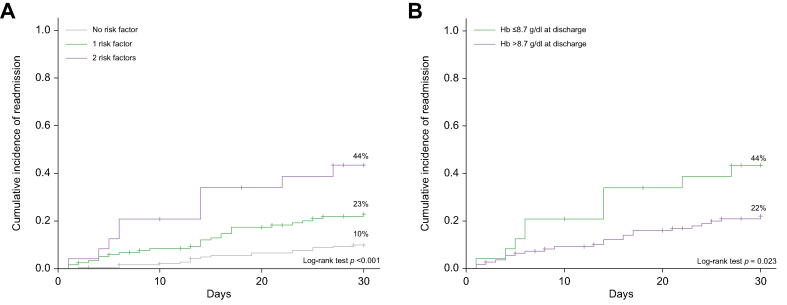
Results: A total of 329 patients with AD were included in the analysis. Acute-on-chronic liver failure was diagnosed in 19% of patients at admission or developed in an additional 9% of patients during the index hospitalisation. During the 1-year follow-up, 182 patients (55%) were rehospitalised and 98 (30%) more than once. The most frequent causes of readmission were hepatic encephalopathy (36%), ascites (22%), and infection (21%). Cumulative incidence of readmission was 20% at 30 days, 39% at 90 days, and 63% at 1 year. Fifty-four patients were readmitted for emergent liver-related causes within 30 days. Early readmission was associated with a higher 1-year mortality (47 vs. 32%, p = 0.037). Multivariable Cox regression analysis showed that haemoglobin (Hb) ≤8.7 g/dl (hazard ratio 2.63 [95% CI 1.38-5.02], p = 0.003) and model for end-stage liver disease-sodium score (MELD-Na) >16 at discharge (hazard ratio 2.23 [95% CI 1.27-3.93], p = 0.005), were independent predictors of early readmission. In patients with MELD-Na >16 at discharge, the presence of Hb ≤8.7 g/dl doubles the risk of early rehospitalisation (44% vs. 22%, p = 0.02).
Conclusion: Besides MELD-Na, a low Hb level (Hb ≤8.7 g/dl) at discharge emerged as a new risk factor for early readmission, contributing to identification of patients who require closer surveillance after discharge.
Impact and implications: Patients with decompensated cirrhosis face frequent hospitalisations. In the present study, type and causes of readmissions were analysed during 1-year follow-up in patients discharged after the index hospitalisation for an acute decompensation of the disease. Early (30-day) liver-related readmission was associated with higher 1-year mortality. The model for end-stage liver disease-sodium score and low haemoglobin at discharge were identified as independent risk factors for early readmissions. Haemoglobin emerged as a new easy-to-use parameter associated with early readmission warranting further investigation.
Keywords: Anaemia; Early readmission; Haemoglobin; Hospitalisation; Liver cirrhosis; MELD score; Systemic inflammation.
© 2023 The Authors.
Conflict of interest statement
All authors declare no conflicts of interest that are relevant to the content of this article. Please refer to the accompanying ICMJE disclosure forms for further details.
Figures
Similar articles
-
Hospital readmissions among patients with decompensated cirrhosis.Am J Gastroenterol. 2012 Feb;107(2):247-52. doi: 10.1038/ajg.2011.314. Epub 2011 Sep 20. Am J Gastroenterol. 2012. PMID: 21931378 Free PMC article.
-
Discharge Outcomes of Hospitalized Patients with New Onset Decompensated Cirrhosis.Dig Dis Sci. 2024 Sep;69(9):3220-3225. doi: 10.1007/s10620-024-08574-8. Epub 2024 Jul 31. Dig Dis Sci. 2024. PMID: 39085484 Free PMC article.
-
Role of precipitants in transition of acute decompensation to acute-on-chronic liver failure in patients with HBV-related cirrhosis.JHEP Rep. 2022 Jul 5;4(10):100529. doi: 10.1016/j.jhepr.2022.100529. eCollection 2022 Oct. JHEP Rep. 2022. PMID: 36052222 Free PMC article.
-
Predictors of 1-month and 3-months Hospital Readmissions in Decompensated Cirrhosis: A Prospective Study in a Large Asian Cohort.Ann Hepatol. 2019 Jan-Feb;18(1):30-39. doi: 10.5604/01.3001.0012.7859. Ann Hepatol. 2019. PMID: 31113606
-
Caseworker-assigned discharge plans to prevent hospital readmission for acute exacerbations in children with chronic respiratory illness.Cochrane Database Syst Rev. 2018 Nov 2;11(11):CD012315. doi: 10.1002/14651858.CD012315.pub2. Cochrane Database Syst Rev. 2018. PMID: 30387126 Free PMC article.
Cited by
-
A novel, nurse-led 'one stop' clinic for patients with liver cirrhosis results in fewer liver-related unplanned readmissions and improved survival.BMC Gastroenterol. 2023 Oct 16;23(1):356. doi: 10.1186/s12876-023-02986-y. BMC Gastroenterol. 2023. PMID: 37845625 Free PMC article.
-
Hemoglobin-to-RDW ratio, hemoglobin-to-monocyte ratio, and hemoglobin-to-leukocyte ratio are predictive of 14-day readmission after primary total knee arthroplasty.J Orthop Surg Res. 2024 Oct 26;19(1):688. doi: 10.1186/s13018-024-05116-w. J Orthop Surg Res. 2024. PMID: 39456066 Free PMC article.
-
Acute decompensation of cirrhosis versus acute-on-chronic liver failure: What are the clinical implications?United European Gastroenterol J. 2024 Mar;12(2):194-202. doi: 10.1002/ueg2.12538. Epub 2024 Feb 20. United European Gastroenterol J. 2024. PMID: 38376886 Free PMC article. Review.
References
-
- Sepanlou S.G., Safiri S., Bisignano C., Ikuta K.S., Merat S., Saberifiroozi M., et al. The global, regional, and national burden of cirrhosis by cause in 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet Gastroenterol Hepatol. 2020;5:245–266. - PMC - PubMed
-
- Mumtaz K., Issak A., Porter K., Kelly S., Hanje J., Michaels A.J., et al. Validation of risk score in predicting early readmissions in decompensated cirrhotic patients: a model based on the administrative database. Hepatology. 2019;70:630–639. - PubMed
LinkOut - more resources
Full Text Sources
