

Aqueous deficiency dry eye in post conjunctivitis cicatrization - Effect of deep thermal punctal cautery
- PMID: 37026314
- PMCID: PMC10276737
- DOI: 10.4103/IJO.IJO_2572_22
Aqueous deficiency dry eye in post conjunctivitis cicatrization - Effect of deep thermal punctal cautery
Abstract
Purpose: To evaluate the effect of deep thermal punctal cautery in eyes with post-conjunctivitis cicatrization.
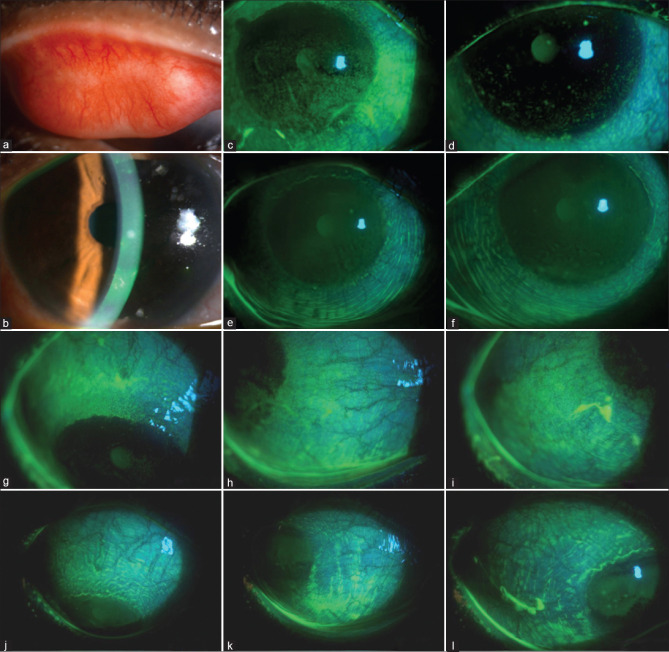
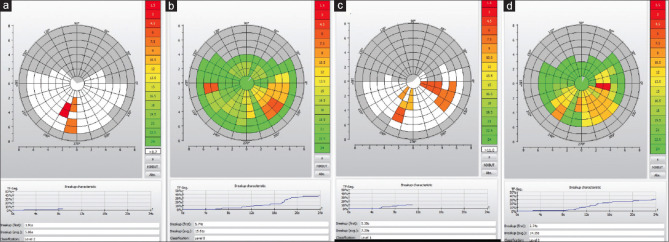
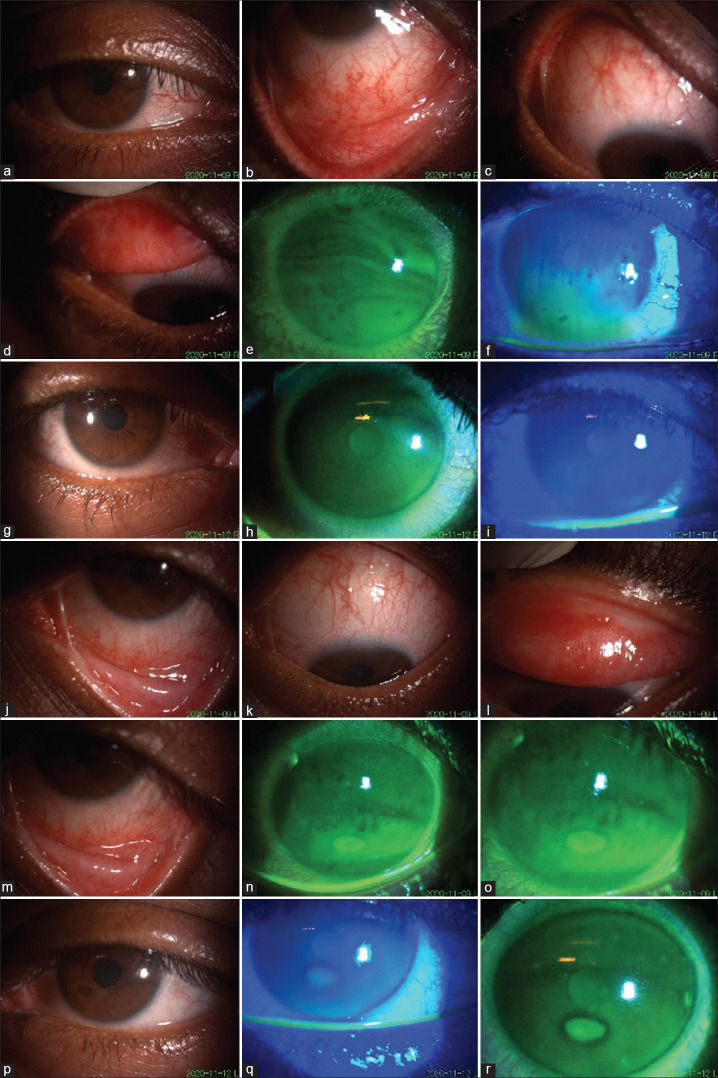
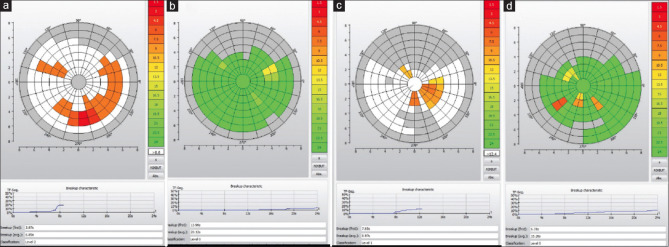
Methods: This retrospective study consisted of patients who underwent deep thermal punctal cautery for post-conjunctivitis dry eye (PCDE). The diagnosis was based on a history suggestive of viral conjunctivitis in past followed by the onset of present clinical features of aqueous deficiency dry eye (ATD). All patients underwent a rheumatological evaluation to rule out underlying systemic collagen vascular disease as a cause for dry eye. The extent of cicatricial changes was noted. Best-corrected visual acuity (BCVA), Schirmer's test, and fluorescein staining score (FSS; total score of 9) were analyzed pre- and post-cautery.
Results: Out of 65 patients (117 eyes), 42 were males. The mean age at presentation was 25.769 ± 12.03 years. Thirteen patients presented with unilateral dry eye. Pre-cautery BCVA (logarithm of the minimum angle of resolution [logMAR]) and Schirmer's test (mm) improved from 0.5251 ± 0.662 to 0.372 ± 0.595 (P value = 0.000, 95% confidence interval [CI]: 0.09-0.22), and 1.952 ± 2.763 to 4.929 ± 4.338 (P value = 0.000, 95% CI: -3.79--2.17); post-cautery, respectively. The pre-cautery FSS of 5.9 ± 2.82 reduced to 1.58 ± 2.38 (P value = 0.000, 95% CI: 3.46-5.17) post-cautery. The mean follow-up was 11.22 ± 13.32 months. No progression in cicatricial changes was noted in any eye during the follow-up. Re-canalization rate was 10.64%, and repeat cautery was performed with successful closure of puncta.
Conclusion: Symptoms and clinical signs of ATD in PCDE patients improve with punctal cautery.
Keywords: Conjunctival cicatricial disease; dry eye; post-conjunctivitis dry eye; punctal cautery.
Conflict of interest statement
None
Figures
Similar articles
-
Surgical management of lacrimal punctal cauterization in chronic GVHD-related dry eye with recurrent punctal plug extrusion.Bone Marrow Transplant. 2012 Nov;47(11):1465-9. doi: 10.1038/bmt.2012.50. Epub 2012 Mar 19. Bone Marrow Transplant. 2012. PMID: 22426754
-
Argon laser punctal therapy versus thermal cautery for the treatment of aqueous deficiency dry eye syndrome.Can J Ophthalmol. 1998 Dec;33(7):365-72. Can J Ophthalmol. 1998. PMID: 9885751 Clinical Trial.
-
Punctal occlusion in the management of chronic Stevens-Johnson syndrome.Ophthalmology. 2004 May;111(5):895-900. doi: 10.1016/j.ophtha.2003.09.034. Ophthalmology. 2004. PMID: 15121365
-
Treatment of dry eye with punctal plugs.Optom Clin. 1991;1(4):103-17. Optom Clin. 1991. PMID: 1799831 Review.
-
Lacrimal duct occlusion for the treatment of dry eye.Semin Ophthalmol. 2005 Apr-Jun;20(2):71-4. doi: 10.1080/08820530590931133. Semin Ophthalmol. 2005. PMID: 16020347 Review.
Cited by
-
Punctal cautery in dry eye disease: A systematic review.Ocul Surf. 2024 Oct;34:235-240. doi: 10.1016/j.jtos.2024.08.006. Epub 2024 Aug 9. Ocul Surf. 2024. PMID: 39127391 Free PMC article.
References
-
- Rajaiya J, Chodosh J. New paradigms in infectious eye disease: adenoviral keratoconjunctivitis. Arch Soc Esp de Oftalmol. 2006;81:493–8. - PubMed
-
- Butt AL, Chodosh J. Adenoviral keratoconjunctivitis in a tertiary care eye clinic. Cornea. 2006;25:199–202. - PubMed
-
- Chiou AG, Florakis GJ, Kazim M. Management of conjunctival cicatrizing diseases and severe ocular surface dysfunction. SurvOphthalmol. 1998;43:19–46. - PubMed
-
- Bron AJ, Abelson MB, Ousler G, Pearce E, Tomlinson A, Yokoi N, et al. Methodologies to diagnose and monitor dry eye disease: Report of the Diagnostic Methodology Subcommittee of the International Dry Eye WorkShop (2007) Ocul Surf. 2007;5:108–52. - PubMed
-
- Ohba E, Dogru M, Hosaka E, Yamazaki A, Asaga R, Tatematsu Y, et al. Surgical punctal occlusion with a high heat-energy releasing cautery device for severe dry eye with recurrent punctal plug extrusion. Am J Ophthalmol. 2011;151:483–7. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
