

Low intra-abdominal pressure in laparoscopic surgery: a systematic review and meta-analysis
- PMID: 37026807
- PMCID: PMC10389627
- DOI: 10.1097/JS9.0000000000000289
Low intra-abdominal pressure in laparoscopic surgery: a systematic review and meta-analysis
Abstract
Background: Guidelines do not provide clear recommendations with regard to the use of low intra-abdominal pressure (IAP) during laparoscopic surgery. The aim of this meta-analysis is to assess the influence of low versus standard IAP during laparoscopic surgery on the key-outcomes in perioperative medicine as defined by the StEP-COMPAC consensus group.
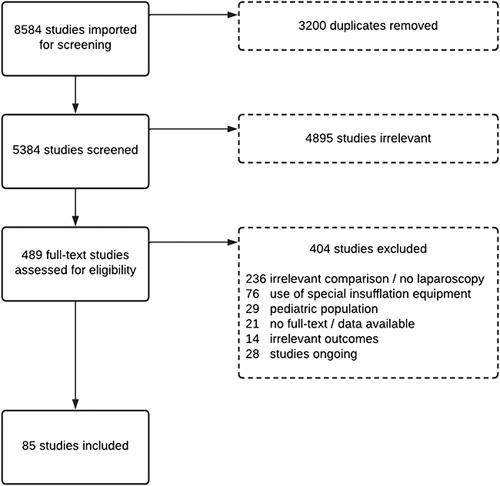
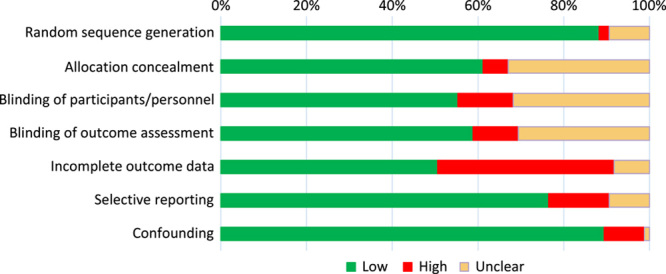
Materials and methods: We searched the Cochrane Library, PubMed, and EMBASE for randomized controlled trials comparing low IAP (<10 mmHg) with standard IAP (10 mmHg or higher) during laparoscopic surgery without time, language, or blinding restrictions. According to the PRISMA guidelines, two review authors independently identified trials and extracted data. Risk ratio (RR), and mean difference (MD), with 95% CIs were calculated using random-effects models with RevMan5. Main outcomes were based on StEP-COMPAC recommendations, and included postoperative complications, postoperative pain, postoperative nausea and vomiting (PONV) scores, and length of hospital stay.
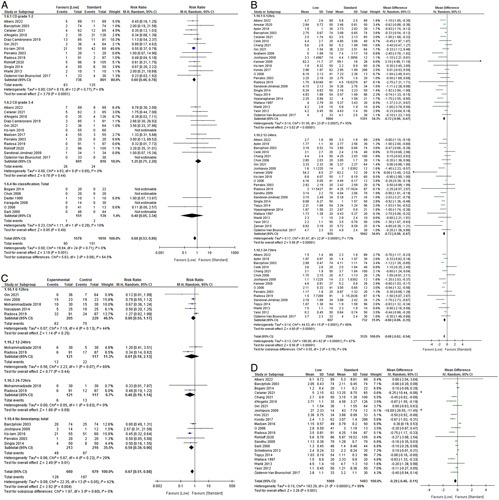
Results: Eighty-five studies in a wide range of laparoscopic procedures (7349 patients) were included in this meta-analysis. The available evidence indicates that the use of low IAP (<10 mmHg) leads to a lower incidence of mild (Clavien-Dindo grade 1-2) postoperative complications (RR=0.68, 95% CI: 0.53-0.86), lower pain scores (MD=-0.68, 95% CI: -0.82 to 0.54) and PONV incidence (RR=0.67, 95% CI: 0.51-0.88), and a reduced length of hospital stay (MD=-0.29, 95% CI: -0.46 to 0.11). Low IAP did not increase the risk of intraoperative complications (RR=1.15, 95% CI: 0.77-1.73).
Conclusions: Given the established safety and the reduced incidence of mild postoperative complications, lower pain scores, reduced incidence of PONV, and shorter length of stay, the available evidence supports a moderate to strong recommendation (1a level of evidence) in favor of low IAP during laparoscopic surgery.
Copyright © 2023 The Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
M.C.W. and O.D.-C. received grants from Merck Sharp & Dohme for investigator-initiated studies. The remaining authors declare that they have no financial conflict of interest with regard to the content of this report.
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.
Figures
References
-
- Neudecker J, Sauerland S, Neugebauer E, et al. The European Association for Endoscopic Surgery clinical practice guideline on the pneumoperitoneum for laparoscopic surgery. Surg Endosc 2002;16:1121–1143. - PubMed
-
- Gustafsson UO, Scott MJ, Hubner M, et al. Guidelines for perioperative care in elective colorectal surgery: Enhanced Recovery After Surgery (ERAS(®)) Society Recommendations: 2018. World J Surg 2019;43:659–695. - PubMed
-
- Nelson G, Bakkum-Gamez J, Kalogera E, et al. Guidelines for perioperative care in gynecologic/oncology: Enhanced Recovery After Surgery (ERAS) Society recommendations-2019 update. Int J Gynecol Cancer 2019;29:651–668. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
