

Management of leaks following one-anastomosis gastric bypass: an updated systematic review and meta-analysis of 44 318 patients
- PMID: 37026835
- PMCID: PMC10389517
- DOI: 10.1097/JS9.0000000000000346
Management of leaks following one-anastomosis gastric bypass: an updated systematic review and meta-analysis of 44 318 patients
Abstract
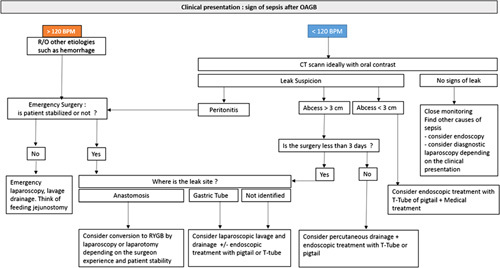
Introduction: One-anastomosis gastric bypass (OAGB) complication, such as leakage, can be dangerous and should be managed properly, yet little data exist in the literature regarding the management of leaks after OAGB, and there are no guidelines to date.
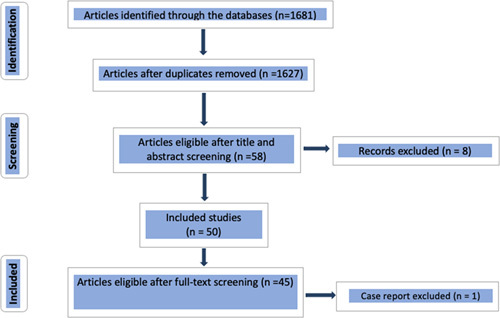
Methods: The authors performed a systematic review and meta-analysis of the literature and 46 studies, examining 44 318 patients were included.
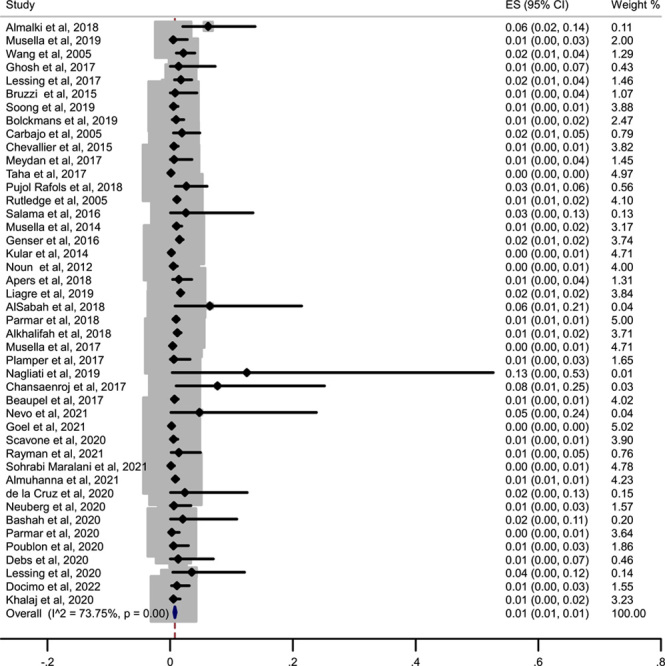
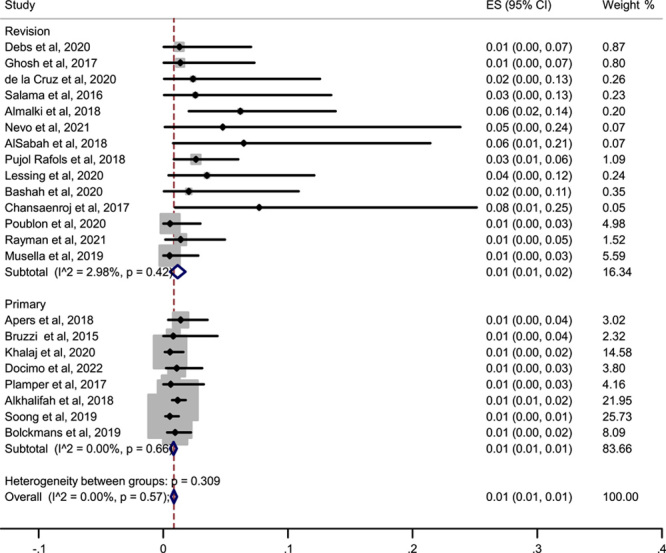
Results: There were 410 leaks reported in 44 318 patients of OAGB published in the literature, which represents a prevalence of 1% of leaks after OAGB. The surgical strategy was very variable among all the different studies; 62.1% of patients with leaks had to undergo another surgery due to the leak. The most commonly performed procedure was peritoneal washout and drainage (with or without T-tube placement) in 30.8% of patients, followed by conversion to Roux-en-Y gastric bypass in 9.6% of patients. Medical treatment with antibiotics, with or without total parenteral nutrition alone, was conducted in 13.6% of patients. Among the patients with the leak, the mortality rate related to the leak was 1.95%, and the mortality due to the leak in the population of OAGB was 0.02%.
Conclusion: The management of leaks following OAGB requires a multidisciplinary approach. OAGB is a safe operation with a low leak risk rate, and the leaks can be managed successfully if detected in a timely fashion.
Copyright © 2023 The Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors declare no conflicts of interest.
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.
Figures
Similar articles
-
Multidisciplinary Management of Leaks After One-Anastomosis Gastric Bypass in a Single-Center Series of 2780 Consecutive Patients.Obes Surg. 2019 May;29(5):1452-1461. doi: 10.1007/s11695-019-03754-2. Obes Surg. 2019. PMID: 30726544
-
Efficiency and risks of laparoscopic conversion of omega anastomosis gastric bypass to Roux-en-Y gastric bypass.Surg Endosc. 2019 Aug;33(8):2572-2582. doi: 10.1007/s00464-018-6552-y. Epub 2018 Oct 23. Surg Endosc. 2019. PMID: 30353237
-
One Anastomosis Gastric Bypass Versus Roux-en-Y Gastric Bypass for Morbid Obesity: an Updated Meta-Analysis.Obes Surg. 2019 Sep;29(9):2721-2730. doi: 10.1007/s11695-019-04005-0. Obes Surg. 2019. PMID: 31172454
-
Endoscopic treatment of early leaks and strictures after laparoscopic one anastomosis gastric bypass.BMC Surg. 2020 Feb 21;20(1):33. doi: 10.1186/s12893-020-0686-2. BMC Surg. 2020. PMID: 32085769 Free PMC article.
-
Randomized Controlled Trial of One Anastomosis Gastric Bypass Versus Roux-En-Y Gastric Bypass for Obesity: Comparison of the YOMEGA and Taiwan Studies.Obes Surg. 2019 Sep;29(9):3047-3053. doi: 10.1007/s11695-019-04065-2. Obes Surg. 2019. PMID: 31290104 Review.
Cited by
-
The role of drain placement in post-bariatric surgery bleeding and leak detection: Palestinian main center experience (2017-2021).BMC Surg. 2025 Apr 7;25(1):138. doi: 10.1186/s12893-025-02884-y. BMC Surg. 2025. PMID: 40189504 Free PMC article.
-
The Safety and Efficacy of Laparoscopic One Anastomosis Gastric Bypass as a Revision for Laparoscopic Adjustable Gastric Banding and Laparoscopic Sleeve Gastrectomy.Obes Surg. 2025 Jul;35(7):2647-2654. doi: 10.1007/s11695-025-07968-5. Epub 2025 Jun 15. Obes Surg. 2025. PMID: 40517361
-
Nonoperative Management Strategies for Anastomotic Leaks After One Anastomosis Gastric Bypass (OAGB): A Literature Review.Cureus. 2024 Sep 19;16(9):e69708. doi: 10.7759/cureus.69708. eCollection 2024 Sep. Cureus. 2024. PMID: 39429265 Free PMC article. Review.
-
One Anastomosis Gastric Bypass in 6722 Patients: Early Outcomes from a Private Hospital Registry.J Clin Med. 2023 Oct 31;12(21):6872. doi: 10.3390/jcm12216872. J Clin Med. 2023. PMID: 37959337 Free PMC article.
-
A New Technique for Jejunal Tube Insertion During Laparoscopic Conversion of One Anastomosis Gastric Bypass (OAGB) to Roux-en-Y Gastric Bypass (RYGB) Due to Anastomosis Leakage.Obes Surg. 2023 Nov;33(11):3712-3713. doi: 10.1007/s11695-023-06871-1. Epub 2023 Oct 7. Obes Surg. 2023. PMID: 37805671 No abstract available.
References
-
- De Luca M, Tie T, Ooi G, et al. . Mini gastric bypass-one anastomosis gastric bypass (MGB-OAGB)-IFSO position statement. Obes Surg 2018;28:1188–1206. - PubMed
-
- Kermansaravi M, Parmar C, Chiappetta S, et al. . Patient selection in one anastomosis/mini gastric bypass – an expert modified Delphi consensus. Obes Surg 2022;32:2512–2524. - PubMed
-
- Kermansaravi M, Shahmiri SS, Davarpanah Jazi AH, et al. . Reversal to normal anatomy after one-anastomosis/mini gastric bypass, indications and results: a systematic review and meta-analysis. Surg Obes Relat Dis 2021;17:1489–1496. - PubMed
-
- Beaupel N, Bruzzi M, Voron T, et al. . Management of acute intra-abdominal sepsis caused by leakage after one anastomosis gastric bypass. Surg Obes Relat Dis 2017;13:1297–1305. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
