

Associations of continuous anionic gap detection with the mortality in critically ill patients receiving renal replacement therapy
- PMID: 37027077
- PMCID: PMC10560184
- DOI: 10.1007/s11255-023-03583-4
Associations of continuous anionic gap detection with the mortality in critically ill patients receiving renal replacement therapy
Abstract
Purpose: To investigate the associations of anion gap (AG) levels before and 1-day after hemodialysis as well as anion gap changes with the mortality in critically ill patients receiving renal replacement therapy (RRT).
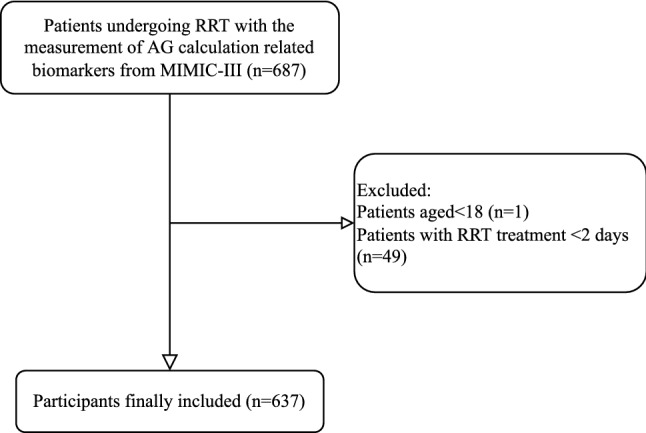
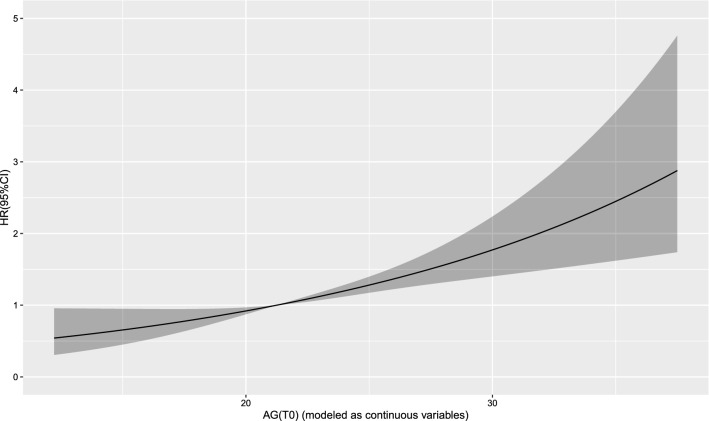
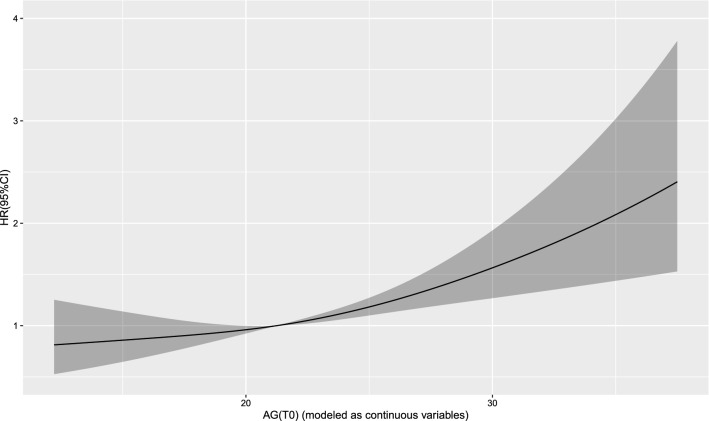
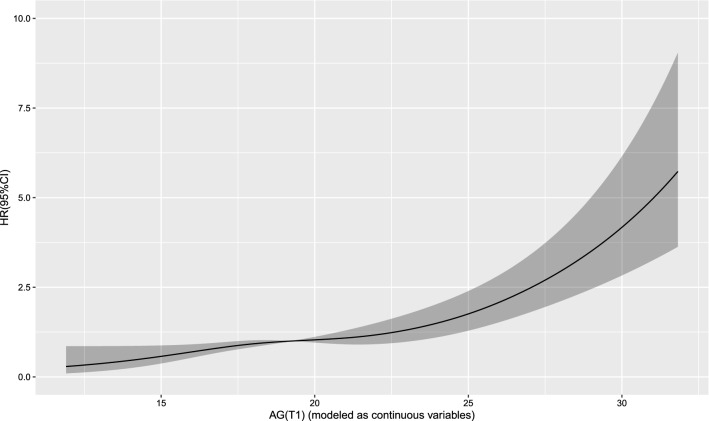
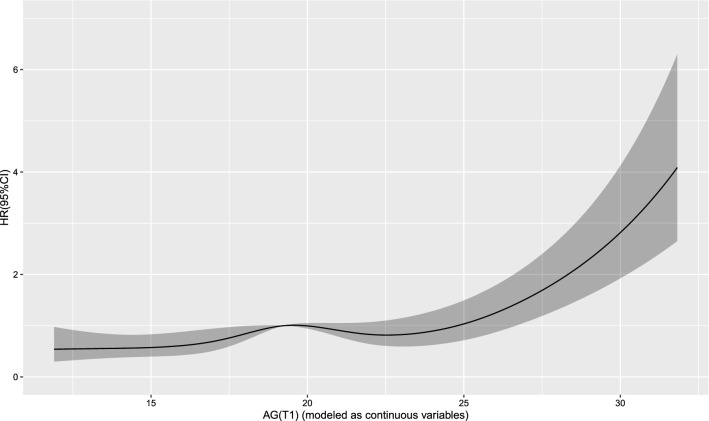
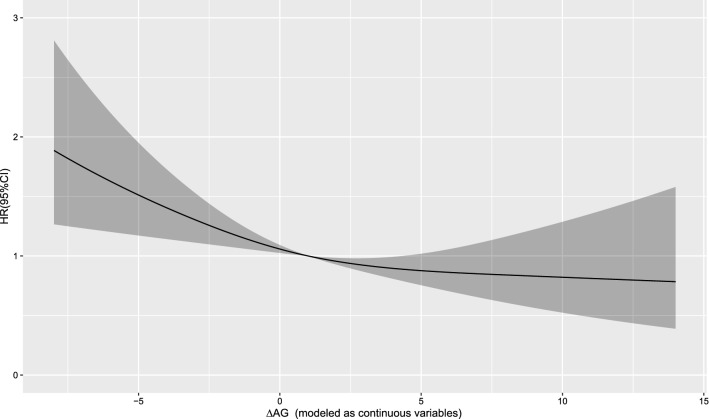
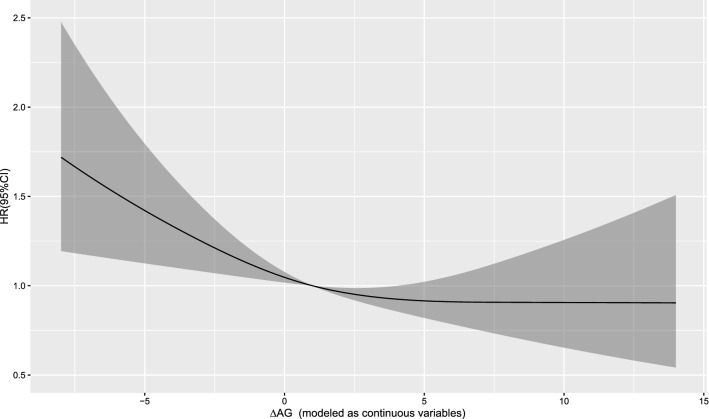
Methods: Totally, 637 patients from MIMIC-III were included in this cohort study. The associations between AG (T0), AG (T1), or ∆AG [AG (T0) - AG (T1)], and the risk of 30-day or 1-year mortality were examined by Cox restricted cubic spline regression models. Univariate and multivariate Cox proportional-hazards model was applied to assess the associations between AG (T0), AG (T1), ∆AG with 30-day and 1-year mortality, respectively.
Results: The median follow-up time was 18.60 (8.53, 38.16) days and 263 (41.3%) patients were survived. There was a linear relationship between AG (T0), AG (T1) or ∆AG and the risk of 30-day or 1-year mortality, respectively. The risk of 30-day mortality was higher in AG (T0) > 21 group (HR = 1.723, 95% CI 1.263-2.350), and AG (T1) > 22.3 group (HR = 2.011, 95% CI 1.417-2.853), while lower in AG > 0 group (HR = 0.664, 95% CI 0.486-0.907). The risk of 1-year mortality was increased in AG (T0) > 21 group (HR = 1.666, 95% CI 1.310-2.119), and AG (T1) > 22.3 group (HR = 1.546, 95% CI 1.159-2.064), while decreased in AG > 0 group (HR = 0.765, 95% CI 0.596-0.981). Patients with AG (T0) ≤ 21 had higher 30-day and 1-year survival probability than those with AG (T0) > 21.
Conclusion: AG before and after dialysis as well as the changes of AG were important factors associated with the risk of 30-day and 1-year mortality in critically ill patients receiving RRT.
Keywords: Dialysis; Renal replacement therapy; Serum anion gap; ∆AG.
© 2023. The Author(s).
Conflict of interest statement
The authors have declared that no conflict of interest exists.
Figures
Similar articles
-
Pre-emptive vs. classic criteria for initiation of dialysis in critically ill patients with acute kidney injury (AKI) - A retrospective real-world study.Hemodial Int. 2023 Jan;27(1):28-37. doi: 10.1111/hdi.13052. Epub 2022 Nov 9. Hemodial Int. 2023. PMID: 36351743
-
Net ultrafiltration intensity and mortality in critically ill patients with fluid overload.Crit Care. 2018 Sep 24;22(1):223. doi: 10.1186/s13054-018-2163-1. Crit Care. 2018. PMID: 30244678 Free PMC article.
-
Effect of Early vs Delayed Initiation of Renal Replacement Therapy on Mortality in Critically Ill Patients With Acute Kidney Injury: The ELAIN Randomized Clinical Trial.JAMA. 2016 May 24-31;315(20):2190-9. doi: 10.1001/jama.2016.5828. JAMA. 2016. PMID: 27209269 Clinical Trial.
-
Accelerated versus standard initiation of renal replacement therapy for critically ill patients with acute kidney injury: a systematic review and meta-analysis of RCT studies.Crit Care. 2021 Jan 5;25(1):5. doi: 10.1186/s13054-020-03434-z. Crit Care. 2021. PMID: 33402204 Free PMC article.
-
Timing of renal replacement therapy initiation for acute kidney injury in critically ill patients: a systematic review of randomized clinical trials with meta-analysis and trial sequential analysis.Crit Care. 2021 Jan 6;25(1):15. doi: 10.1186/s13054-020-03451-y. Crit Care. 2021. PMID: 33407756 Free PMC article.
References
-
- Kim KY, Ryu JH, Kang DH, Kim SJ, Choi KB, Lee S. Early fluid management affects short-term mortality in patients with end-stage kidney disease undergoing chronic hemodialysis and requiring continuous renal replacement therapy. BMC Nephrol. 2022;23(1):102. doi: 10.1186/s12882-022-02725-7. - DOI - PMC - PubMed
-
- Naorungroj T, Neto AS, Yanase F, Eastwood G, Wald R, Bagshaw SM, Bellomo R. Time to initiation of renal replacement therapy among critically ill patients with acute kidney injury: a current systematic review and meta-analysis. Crit Care Med. 2021;49(8):e781–e792. doi: 10.1097/ccm.0000000000005018. - DOI - PubMed
-
- Woodward CW, Lambert J, Ortiz-Soriano V, Li Y, Ruiz-Conejo M, Bissell BD, Kelly A, Adams P, Yessayan L, Morris PE, Neyra JA. Fluid overload associates with major adverse kidney events in critically ill patients with acute kidney injury requiring continuous renal replacement therapy. Crit Care Med. 2019;47(9):e753–e760. doi: 10.1097/ccm.0000000000003862. - DOI - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
