

Bipolar Androgen Therapy Followed by Androgen Receptor Inhibition as Sequential Therapy for Prostate Cancer
- PMID: 37027449
- PMCID: PMC10243791
- DOI: 10.1093/oncolo/oyad055
Bipolar Androgen Therapy Followed by Androgen Receptor Inhibition as Sequential Therapy for Prostate Cancer
Abstract
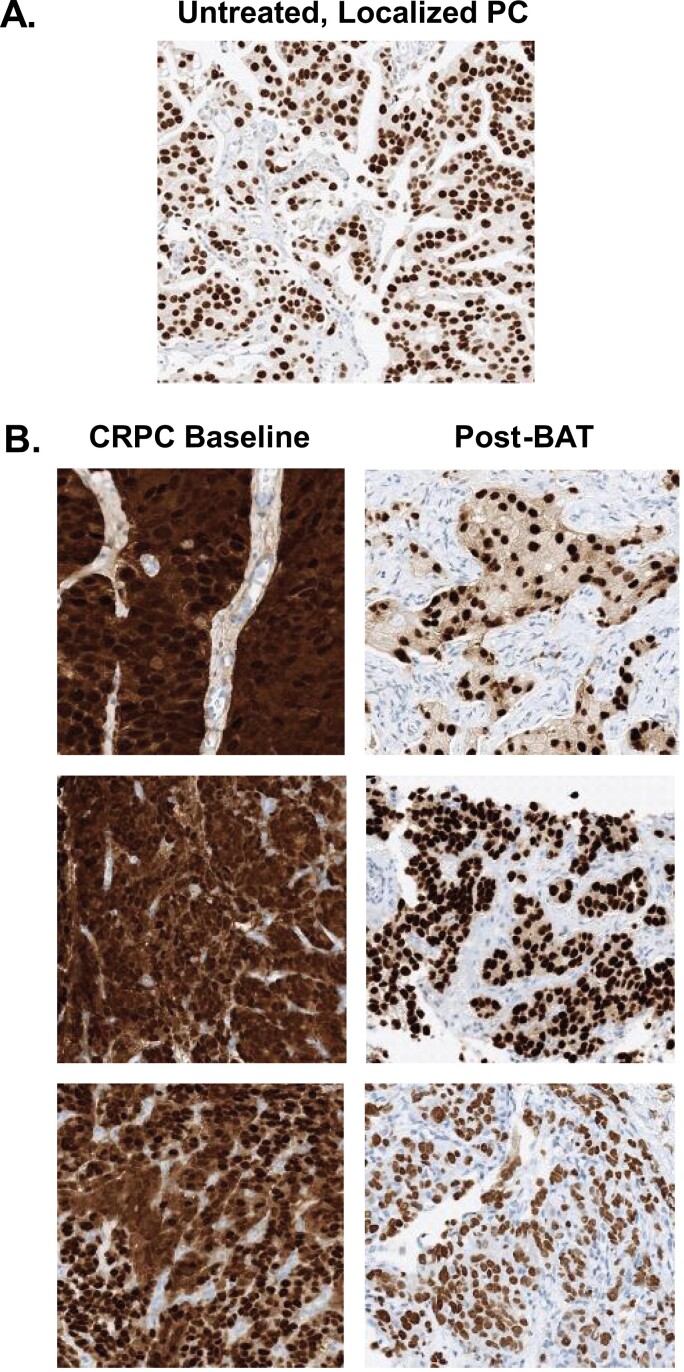
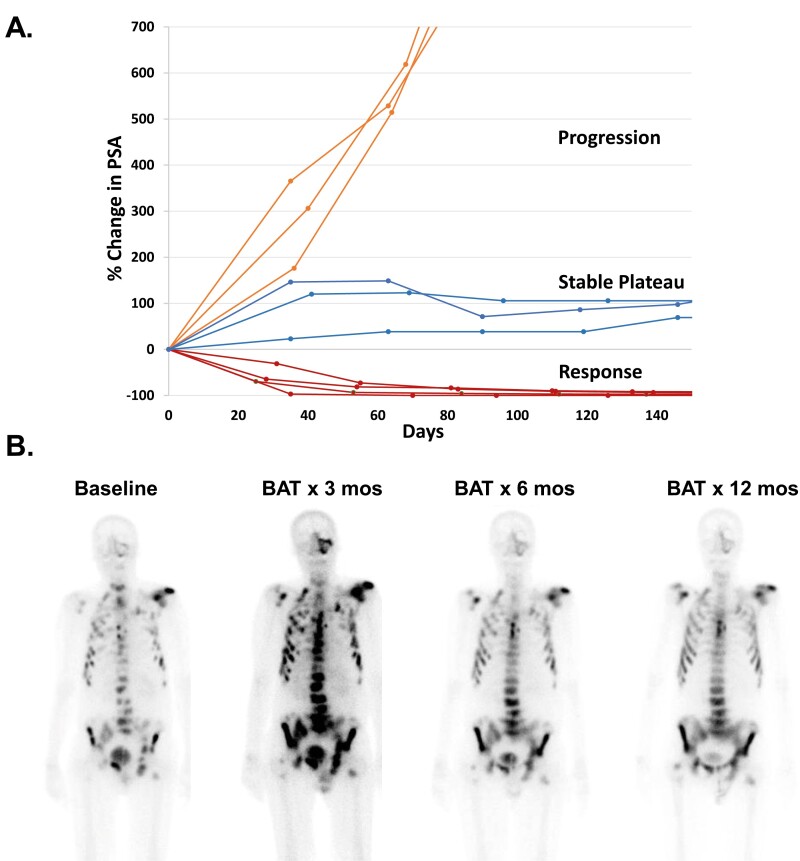
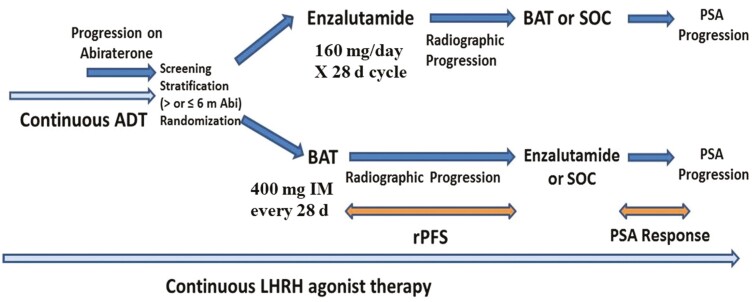
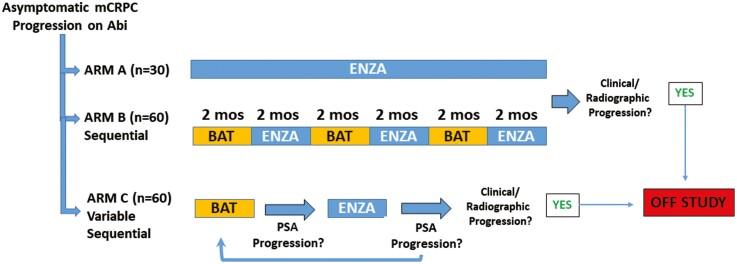
Inhibition of androgen receptor (AR) signaling has been the mainstay of treatment of advanced prostate cancer (PCa) for the past 80 years. Combination and sequential AR-inhibiting therapies are highly effective palliative therapy, but they are not curative. All patients eventually develop resistance to primary castrating therapy [ie, castration-resistant PCa (CRPC)]. At this point, they are treated with subsequent lines of secondary AR inhibitory therapies. However, resistance to these agents also develops and patients progress to a state we have termed complete androgen inhibition-resistant PCa. This phase of the disease is associated with poor prognosis. At this point, treatment shifts to non-hormonal cytotoxic therapies (eg, chemotherapy and radiopharmaceuticals). However, the majority of PCas remain addicted to signaling through AR throughout the course of the disease. Resistant PCa cells adaptively upregulate AR activity, despite castration and AR inhibitors, via mechanisms such as AR overexpression, gene amplification, mutation, and expression of ligand-independent variants to permit sustained liganded and non-liganded AR signaling. Studies dating back nearly 30 years indicate that high expression of AR induced by prolonged castration becomes a vulnerability of CRPC cells in vitro and in mouse xenografts to supraphysiologic androgen (SPA), which induces cell death and growth arrest in this context. Based on these studies, we developed a counterintuitive treatment called bipolar androgen therapy (BAT) for patients with CRPC, in which SPA is administered intermittently to result in cycling of serum testosterone from the polar extremes of supraphysiologic to near-castrate levels. This rapid cycling is intended to disrupt the adaptive of AR regulation associated with chronic exposure to high or low levels of testosterone, while simultaneously targeting the spectrum of AR expression present in heterogeneous CRPC tumors. We have now tested BAT in >250 patients with CRPC. Here we present a review of these clinical studies, which have demonstrated collectively that BAT can be safely given to men with CRPC, improves quality of life, and produces therapeutic responses in ~30% of patients. As expected, resistance to BAT is associated with adaptive downregulation of AR expression. Intriguingly, this downregulation is associated with restoration of sensitivity to subsequent AR inhibitor therapies.
Keywords: androgen receptor; bipolar androgen therapy; castration-resistant; prostate cancer.
© The Author(s) 2023. Published by Oxford University Press.
Conflict of interest statement
The authors declare the following financial interests/personal relationships which may be considered as potential competing interests: Samuel R. Denmeade has received research funding to his institution from Astellas. Emmanuel S. Antonarakis is a paid consultant/adviser to Janssen, Astellas, Sanofi, Dendreon, Pfizer, Amgen, Lilly, Bayer, AstraZeneca, Bristol-Myers Squibb, Clovis, and Merck; he has received research funding to his institution from Janssen, Johnson & Johnson, Sanofi, Dendreon, Genentech, Novartis, Tokai, Bristol Myers-Squibb, AstraZeneca, Clovis, and Merck; and he is the co-inventor of an AR-V7 biomarker technology that has been licensed to Qiagen. Mark C. Markowski is a paid consultant to Clovis and Exelixis. Laura A. Sena and Hao Wang indicated no financial relationships.
Figures
Similar articles
-
Effect of bipolar androgen therapy for asymptomatic men with castration-resistant prostate cancer: results from a pilot clinical study.Sci Transl Med. 2015 Jan 7;7(269):269ra2. doi: 10.1126/scitranslmed.3010563. Sci Transl Med. 2015. PMID: 25568070 Free PMC article. Clinical Trial.
-
Androgen receptors in hormone-dependent and castration-resistant prostate cancer.Pharmacol Ther. 2013 Dec;140(3):223-38. doi: 10.1016/j.pharmthera.2013.07.003. Epub 2013 Jul 13. Pharmacol Ther. 2013. PMID: 23859952 Review.
-
Bipolar androgen therapy sensitizes castration-resistant prostate cancer to subsequent androgen receptor ablative therapy.Eur J Cancer. 2021 Feb;144:302-309. doi: 10.1016/j.ejca.2020.11.043. Epub 2020 Dec 29. Eur J Cancer. 2021. PMID: 33383350 Free PMC article. Clinical Trial.
-
Androgen receptor functions in castration-resistant prostate cancer and mechanisms of resistance to new agents targeting the androgen axis.Oncogene. 2014 May 29;33(22):2815-25. doi: 10.1038/onc.2013.235. Epub 2013 Jun 10. Oncogene. 2014. PMID: 23752196 Free PMC article. Review.
-
Abiraterone switches castration-resistant prostate cancer dependency from adrenal androgens towards androgen receptor variants and glucocorticoid receptor signalling.Prostate. 2022 Apr;82(5):505-516. doi: 10.1002/pros.24297. Epub 2022 Jan 17. Prostate. 2022. PMID: 35037287 Free PMC article.
Cited by
-
Epigenetic disruption of the RARγ complex impairs its function to bookmark AR enhancer interactions required for enzalutamide sensitivity in prostate cancer.bioRxiv [Preprint]. 2024 Feb 5:2023.12.15.571947. doi: 10.1101/2023.12.15.571947. bioRxiv. 2024. PMID: 38168185 Free PMC article. Preprint.
-
Mediator kinase inhibition reverses castration resistance of advanced prostate cancer.J Clin Invest. 2024 Mar 28;134(10):e176709. doi: 10.1172/JCI176709. J Clin Invest. 2024. PMID: 38546787 Free PMC article.
-
Opposing impact of hypertension/diabetes following hormone therapy initiation and preexisting statins on castration resistant progression of nonmetastatic prostate cancer: a multicenter study.Sci Rep. 2024 Oct 4;14(1):23119. doi: 10.1038/s41598-024-73197-y. Sci Rep. 2024. PMID: 39367145 Free PMC article.
References
-
- Huggins C, Hodges CV.. Studies on prostatic cancer. I. The effect of castration, of estrogen and androgen injection on serum phosphatases in metastatic carcinoma of the prostate. Cancer Res. 1941;1(1):293-297. - PubMed
-
- Huggins C, Stevens RE, Hodges CV. Studies on prostate canceer II: The effects of castration on advanced carcinoma of the prostate gland. Arch Surg. 1941;43(August):209-223.
-
- Denmeade SR. “Androgens”. In: Bast RC, Kuff DW, Pollock RE, Weichelbaum RR, Holland JF, Frei E, eds. Cancer Medicine. 8th ed. Hamilton, Ontario: B.C. Decker, Inc.;2011.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
