

Gene editing to prevent ventricular arrhythmias associated with cardiomyocyte cell therapy
- PMID: 37028405
- PMCID: PMC10283080
- DOI: 10.1016/j.stem.2023.03.010
Gene editing to prevent ventricular arrhythmias associated with cardiomyocyte cell therapy
Erratum in
-
Gene editing to prevent ventricular arrhythmias associated with cardiomyocyte cell therapy.Cell Stem Cell. 2023 May 4;30(5):741. doi: 10.1016/j.stem.2023.04.010. Cell Stem Cell. 2023. PMID: 37146587 Free PMC article. No abstract available.
Abstract
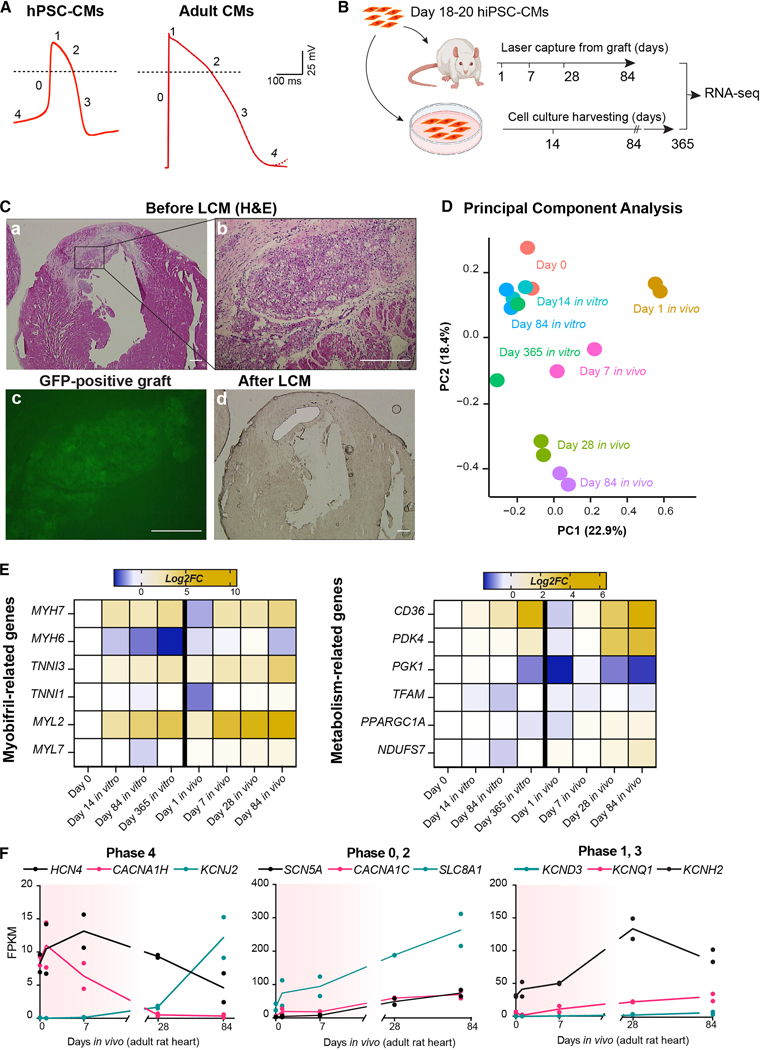
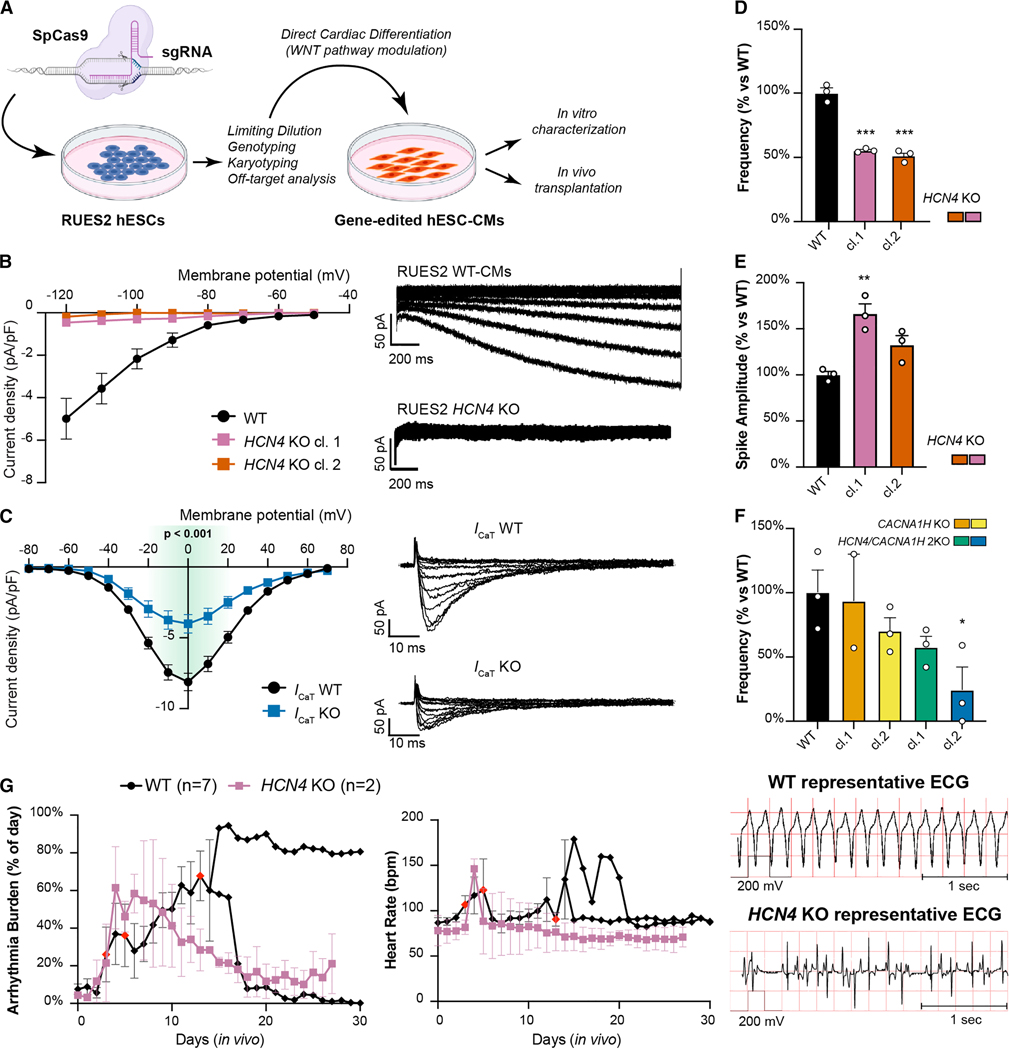
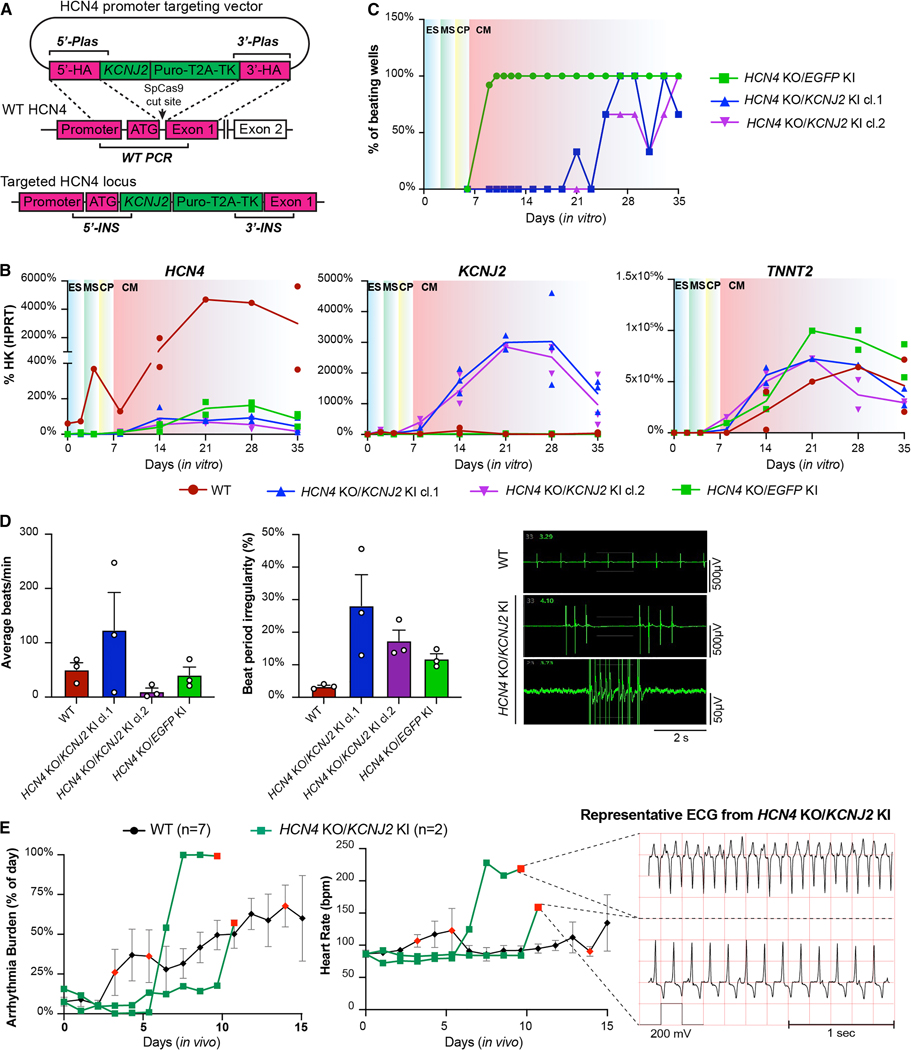
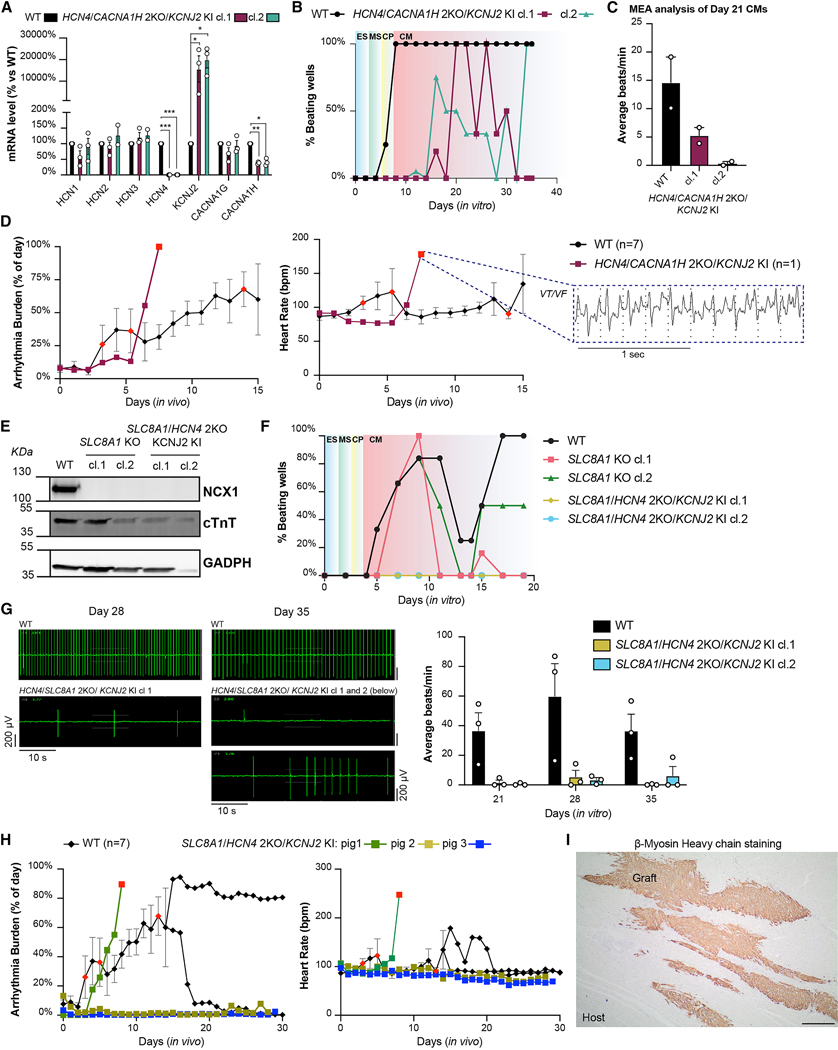
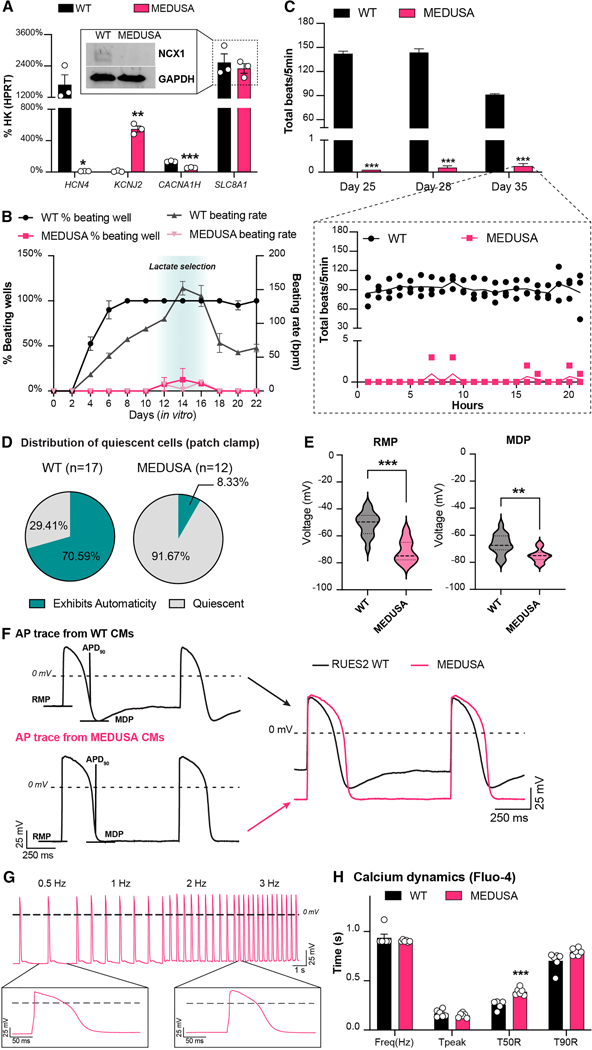
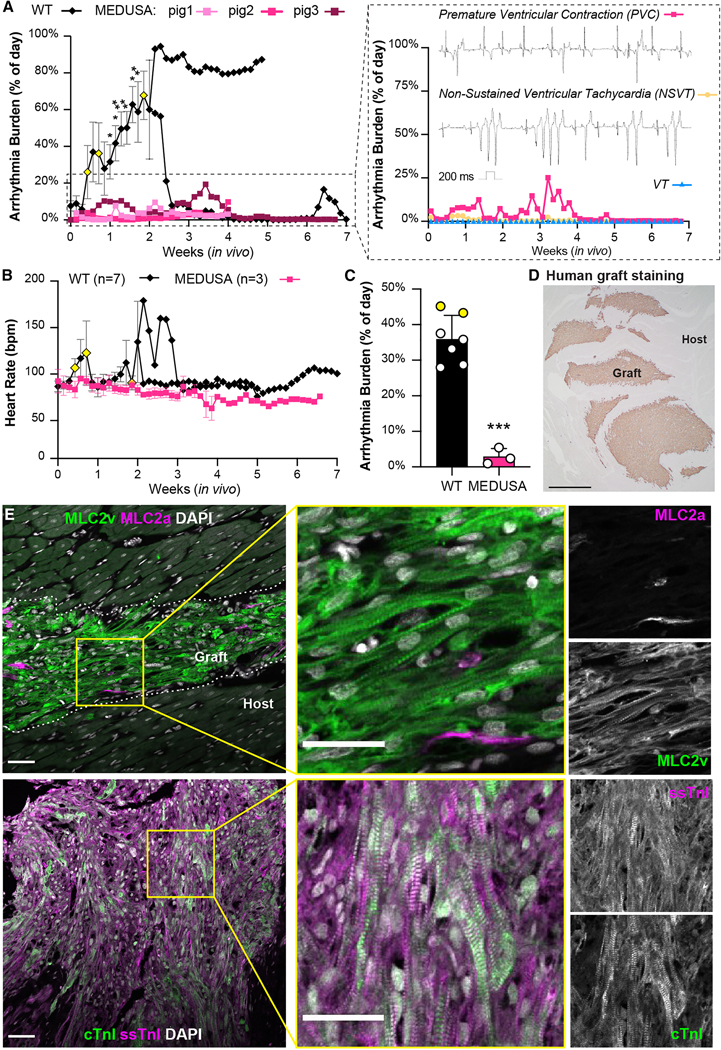
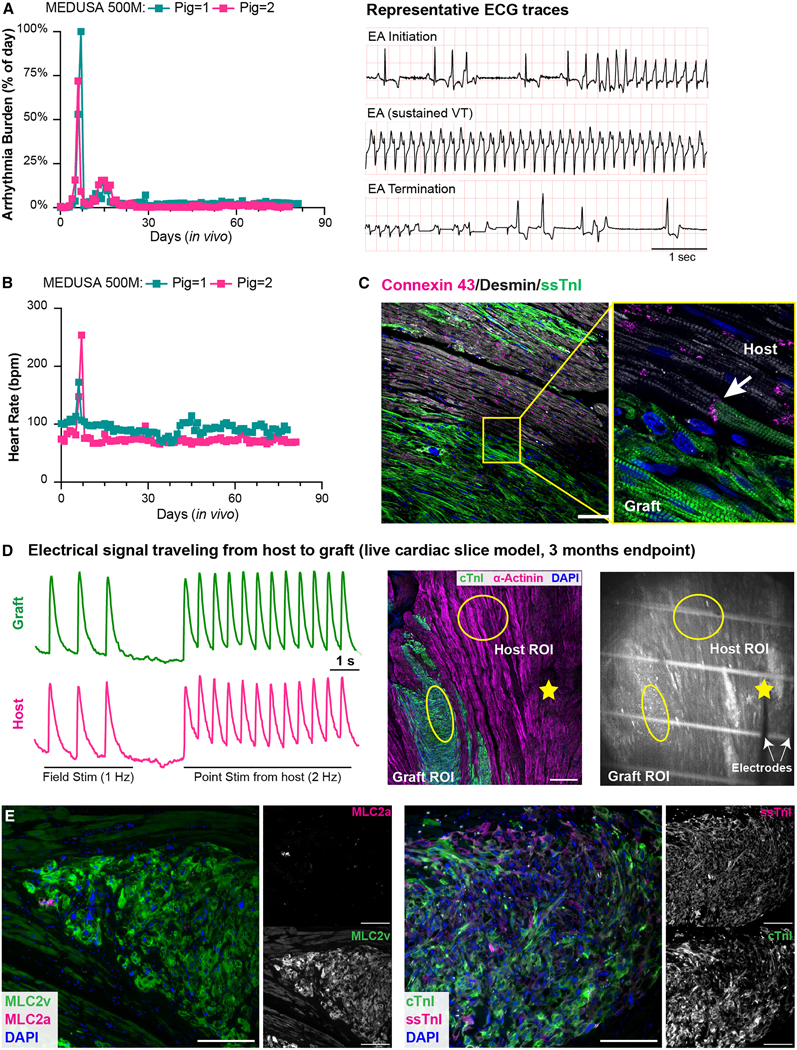
Human pluripotent stem cell-derived cardiomyocytes (hPSC-CMs) offer a promising cell-based therapy for myocardial infarction. However, the presence of transitory ventricular arrhythmias, termed engraftment arrhythmias (EAs), hampers clinical applications. We hypothesized that EA results from pacemaker-like activity of hPSC-CMs associated with their developmental immaturity. We characterized ion channel expression patterns during maturation of transplanted hPSC-CMs and used pharmacology and genome editing to identify those responsible for automaticity in vitro. Multiple engineered cell lines were then transplanted in vivo into uninjured porcine hearts. Abolishing depolarization-associated genes HCN4, CACNA1H, and SLC8A1, along with overexpressing hyperpolarization-associated KCNJ2, creates hPSC-CMs that lack automaticity but contract when externally stimulated. When transplanted in vivo, these cells engrafted and coupled electromechanically with host cardiomyocytes without causing sustained EAs. This study supports the hypothesis that the immature electrophysiological prolife of hPSC-CMs mechanistically underlies EA. Thus, targeting automaticity should improve the safety profile of hPSC-CMs for cardiac remuscularization.
Keywords: arrhythmia; automaticity; cardiac remuscularization; cell therapy; engraftment arrhythmia; hPSC-CM maturation; heart regeneration; human pluripotent stem cell-derived cardiomyocytes; myocardial infarction; pacemaker.
Copyright © 2023 Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of interests K.N., B.C.K., and W.R.M. were advisors to Sana Biotechnology. M.L., A.J., F.A.K., A.F.T., S.D., H.T., L.P., S.K., R.S.T., and C.E.M. were employees while part of this study was performed and continue to hold equity in Sana Biotechnology. S.M., H.R., A.B., and C.E.M. have submitted a provisional patent application pertaining to the work in this manuscript (PCT/US2022/027382).
Figures
Comment in
-
When gene editing turns a nasty goddess into a friendly MEDUSA.Cell Stem Cell. 2023 Apr 6;30(4):340-342. doi: 10.1016/j.stem.2023.03.006. Cell Stem Cell. 2023. PMID: 37028399
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
