

Data-driven analysis to understand long COVID using electronic health records from the RECOVER initiative
- PMID: 37029117
- PMCID: PMC10080528
- DOI: 10.1038/s41467-023-37653-z
Data-driven analysis to understand long COVID using electronic health records from the RECOVER initiative
Abstract
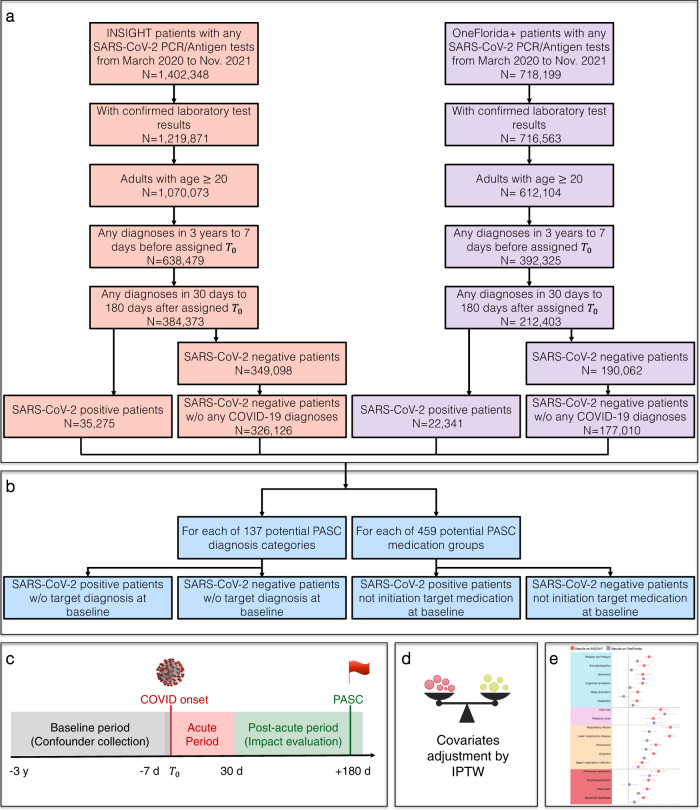
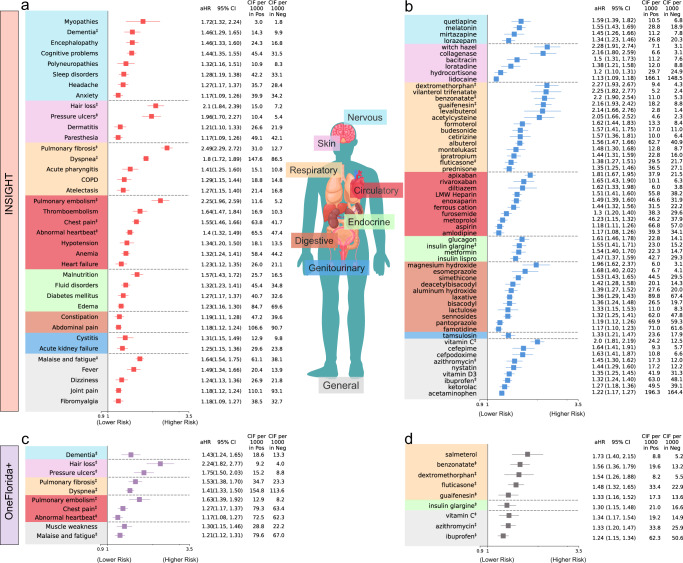
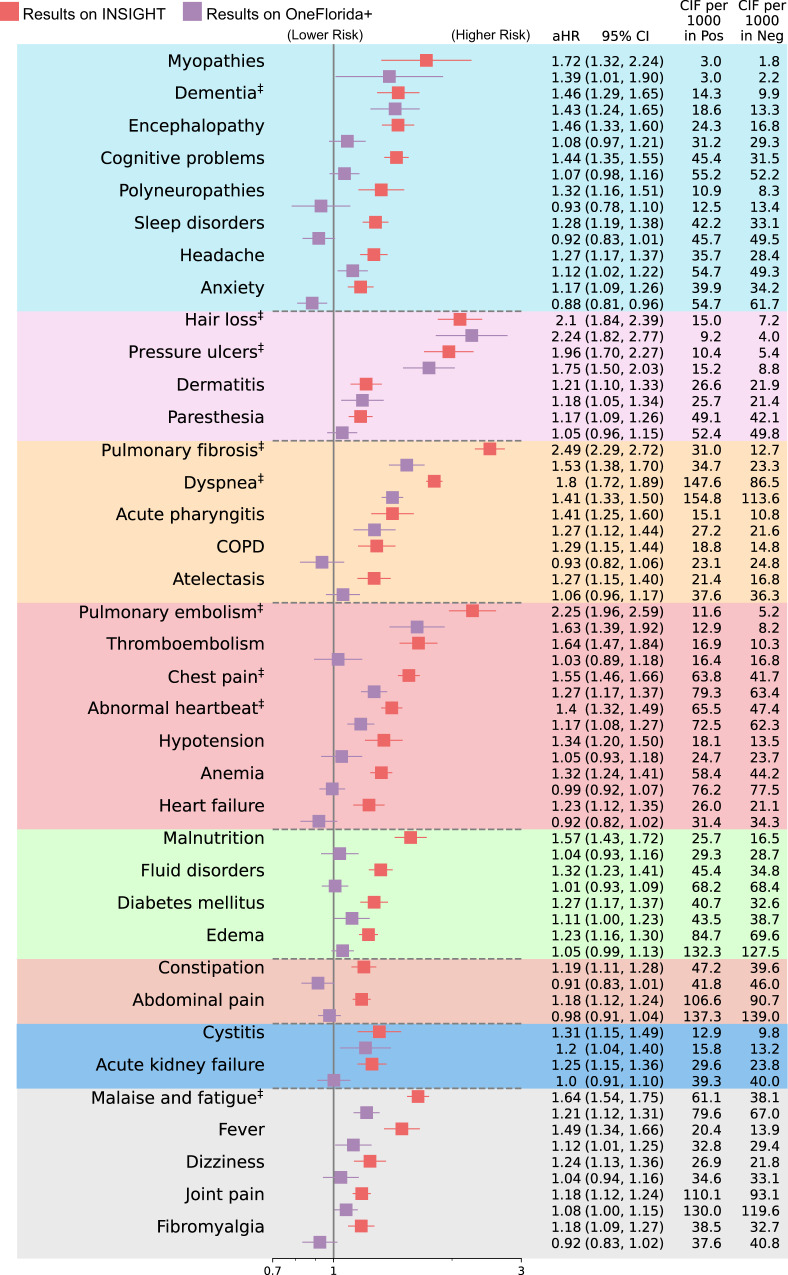
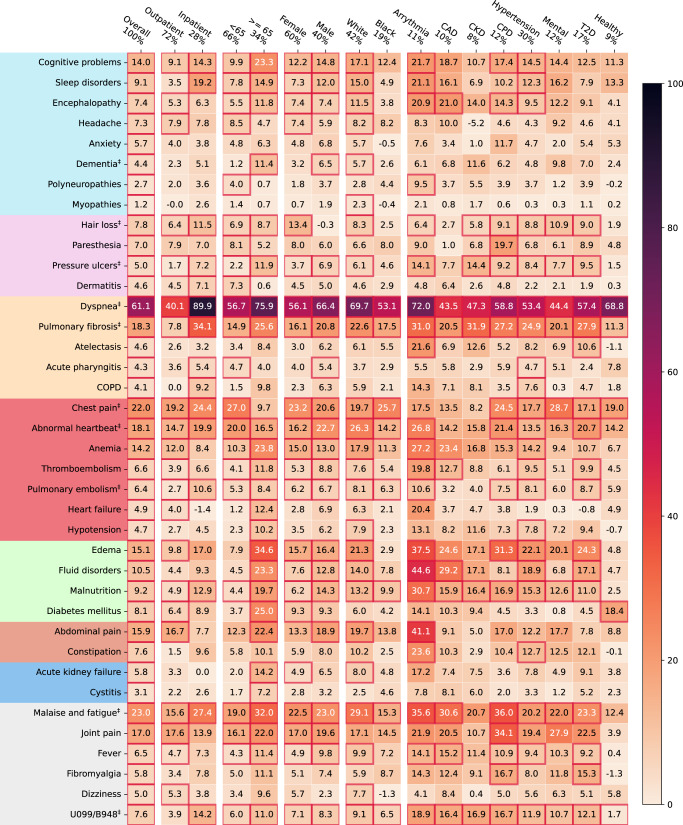
Recent studies have investigated post-acute sequelae of SARS-CoV-2 infection (PASC, or long COVID) using real-world patient data such as electronic health records (EHR). Prior studies have typically been conducted on patient cohorts with specific patient populations which makes their generalizability unclear. This study aims to characterize PASC using the EHR data warehouses from two large Patient-Centered Clinical Research Networks (PCORnet), INSIGHT and OneFlorida+, which include 11 million patients in New York City (NYC) area and 16.8 million patients in Florida respectively. With a high-throughput screening pipeline based on propensity score and inverse probability of treatment weighting, we identified a broad list of diagnoses and medications which exhibited significantly higher incidence risk for patients 30-180 days after the laboratory-confirmed SARS-CoV-2 infection compared to non-infected patients. We identified more PASC diagnoses in NYC than in Florida regarding our screening criteria, and conditions including dementia, hair loss, pressure ulcers, pulmonary fibrosis, dyspnea, pulmonary embolism, chest pain, abnormal heartbeat, malaise, and fatigue, were replicated across both cohorts. Our analyses highlight potentially heterogeneous risks of PASC in different populations.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- WHO. Coronavirus Disease (COVID-19). https://www.who.int/emergencies/diseases/novel-coronavirus-2019 (2023).
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
