

Risk factors and a novel cerebral infarction extent scoring system for postoperative cerebral ischemia in patients with ischemic Moyamoya disease
- PMID: 37029162
- PMCID: PMC10082086
- DOI: 10.1038/s41598-022-26985-3
Risk factors and a novel cerebral infarction extent scoring system for postoperative cerebral ischemia in patients with ischemic Moyamoya disease
Abstract
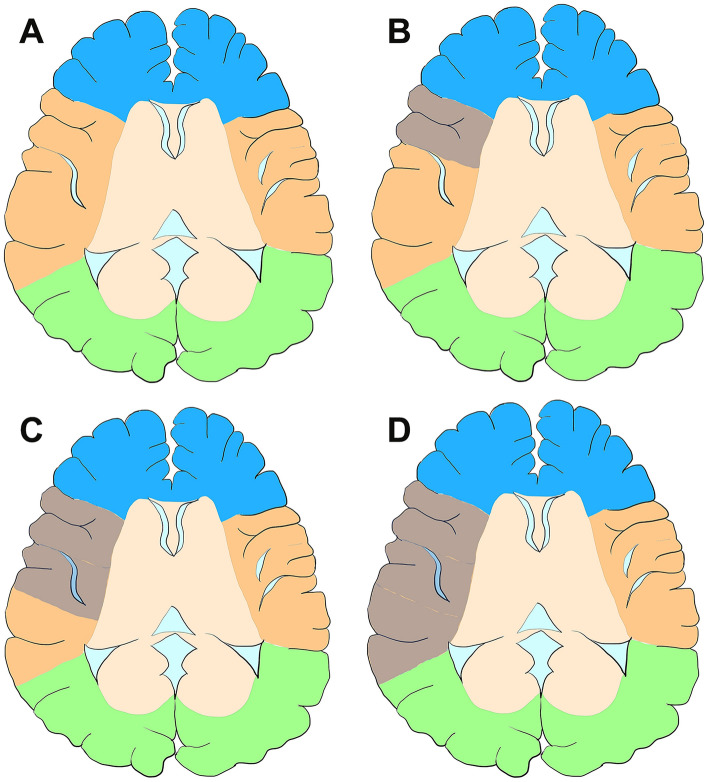
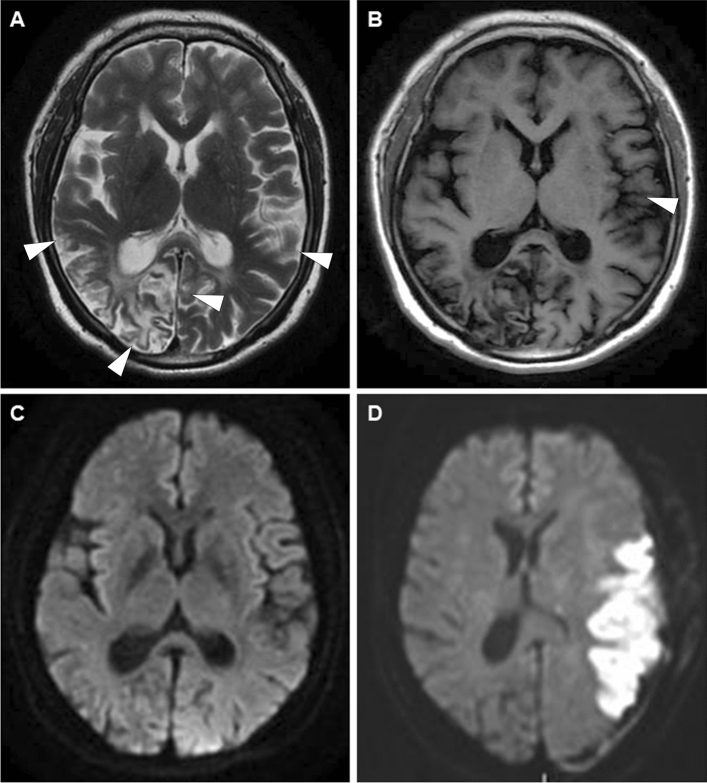
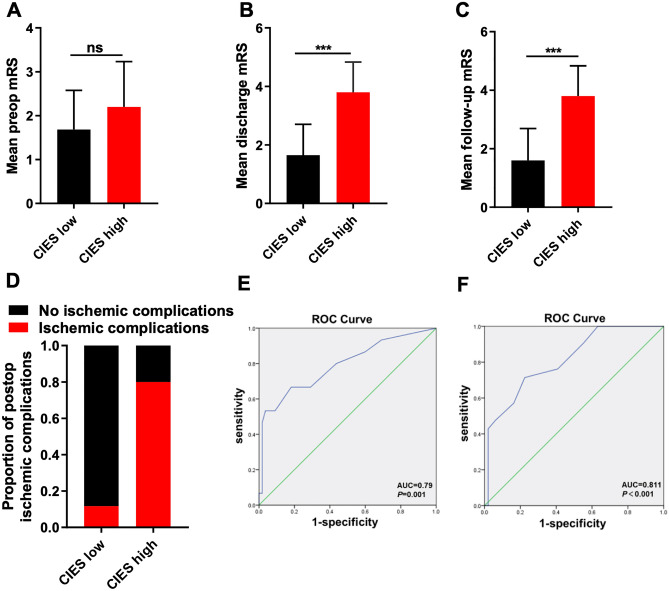
Postoperative cerebral ischemic complication is the most common complication of revascularization surgery for patients with moyamoya disease (MMD). This retrospective study was conducted on 63 patients with ischemic MMD. Postoperative ischemia occurred in 15 of the 70 revascularization operations performed for patients after surgical revascularization, translating to an incidence of 21.4%. Univariate analysis revealed that onset infarction (p = 0.015), posterior cerebral artery involvement (p = 0.039), strict perioperative management (p = 0.001), interval time between transient ischemic attack (TIA) or infarction presentation and operation (p = 0.002) and preoperatively cerebral infarction extent score (CIES) (p = 0.002) were significantly associated with postoperative cerebral ischemia. Multivariate analysis revealed that strict perioperative management (OR = 0.163; p = 0.047), and preoperatively CIES (OR = 1.505; p = 0.006) were independently associated with postoperative cerebral ischemia-related complications. After comprehensive improvement of perioperative management protocol, the incidence of symptomatic infarction declined to 7.4% (4 out of 54). Analysis of the area under the receiver operating characteristic curve (AUROC) indicated CIES was a predictor for both postoperative ischemia and high follow-up modified Rankin Scale scores. In summary, strict perioperative management and CIES were identified as independent risk factors for postoperative ischemic complications in ischemic MMD, demonstrating that comprehensive and individualized perioperative management improve postoperative outcomes in patients with MMD. Furthermore, application of CIES to evaluate pre-existing cerebral infarction can improve the management of patients.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


Similar articles
-
Risk Factors for Newly Developed Cerebral Infarction After Surgical Revascularization for Adults with Moyamoya Disease.World Neurosurg. 2016 Aug;92:65-73. doi: 10.1016/j.wneu.2016.03.053. Epub 2016 Mar 26. World Neurosurg. 2016. PMID: 27020972
-
Development and validation of machine learning models to predict postoperative infarction in moyamoya disease.J Neurosurg. 2024 Apr 5;141(4):927-935. doi: 10.3171/2024.1.JNS232173. Print 2024 Oct 1. J Neurosurg. 2024. PMID: 38579355
-
Unstable moyamoya disease: clinical features and impact on perioperative ischemic complications.J Neurosurg. 2015 Feb;122(2):400-7. doi: 10.3171/2014.10.JNS14231. Epub 2014 Nov 28. J Neurosurg. 2015. PMID: 25423271
-
Progress on Complications of Direct Bypass for Moyamoya Disease.Int J Med Sci. 2016 Jul 5;13(8):578-87. doi: 10.7150/ijms.15390. eCollection 2016. Int J Med Sci. 2016. PMID: 27499690 Free PMC article. Review.
-
Risk factors for postoperative stroke in adults patients with moyamoya disease: a systematic review with meta-analysis.BMC Neurol. 2019 May 15;19(1):98. doi: 10.1186/s12883-019-1327-1. BMC Neurol. 2019. PMID: 31092214 Free PMC article.
Cited by
-
Development and validation of a scoring system to evaluate and clinically manage postoperative acute infarction complications in moyamoya disease.Commun Med (Lond). 2025 Jun 4;5(1):215. doi: 10.1038/s43856-025-00937-0. Commun Med (Lond). 2025. PMID: 40467870 Free PMC article.
-
Introducing an index on prediction of post-revascularization cerebral infarction using preoperative CT perfusion parameters in moyamoya disease.Insights Imaging. 2025 Jan 2;16(1):2. doi: 10.1186/s13244-024-01882-7. Insights Imaging. 2025. PMID: 39747722 Free PMC article.
-
Prediction of cerebral infarction after bypass surgery in adult moyamoya disease: combing parameters on 4D perfusion CT with clinical related factors.Acta Neurochir (Wien). 2024 Nov 28;166(1):484. doi: 10.1007/s00701-024-06373-8. Acta Neurochir (Wien). 2024. PMID: 39607649 Free PMC article.
-
Effect of newly developed scissors-attached micro-forceps on the recipient clamp time and occurrence of anastomotic site infarction after bypass surgery for moyamoya disease.Front Neurol. 2023 Oct 6;14:1269400. doi: 10.3389/fneur.2023.1269400. eCollection 2023. Front Neurol. 2023. PMID: 37869149 Free PMC article.
References
Publication types
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
