

Genomic landscape and clinical features of rare subtypes of pancreatic cancer: analysis with the national database of Japan
- PMID: 37029223
- PMCID: PMC10199859
- DOI: 10.1007/s00535-023-01986-9
Genomic landscape and clinical features of rare subtypes of pancreatic cancer: analysis with the national database of Japan
Abstract
Background: Special subtypes of pancreatic cancer, such as acinar cell carcinoma (ACC), adenosquamous carcinoma (ASC), and anaplastic carcinoma of the pancreas (ACP), are rare, and so data on them are limited. Using the C-CAT database, we analyzed clinical and genomic characteristics of patients with these and evaluated differences on comparison with pancreatic ductal adenocarcinoma (PDAC) patients.
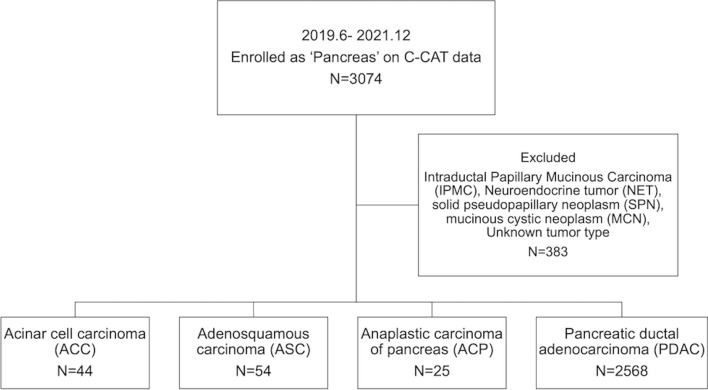
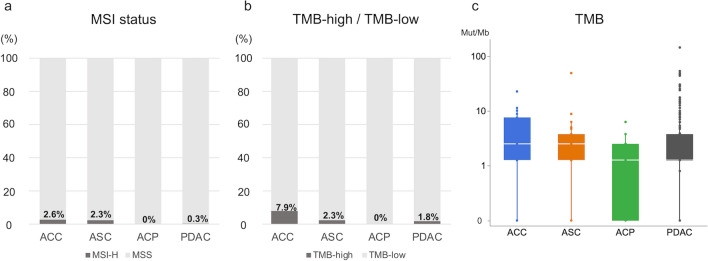
Methods: We retrospectively reviewed data on 2691 patients with unresectable pancreatic cancer: ACC, ASC, ACP, and PDAC, entered into C-CAT from June 2019 to December 2021. The clinical features, MSI/TMB status, genomic alterations, overall response rate (ORR), disease control rate (DCR), and time to treatment failure (TTF) on receiving FOLFIRINOX (FFX) or GEM + nab-PTX (GnP) therapy as first-line treatment were evaluated.
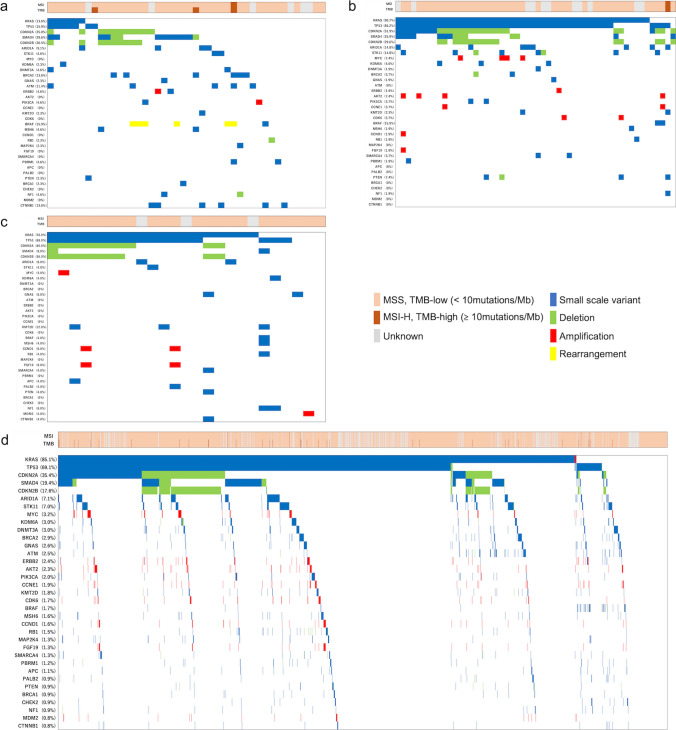
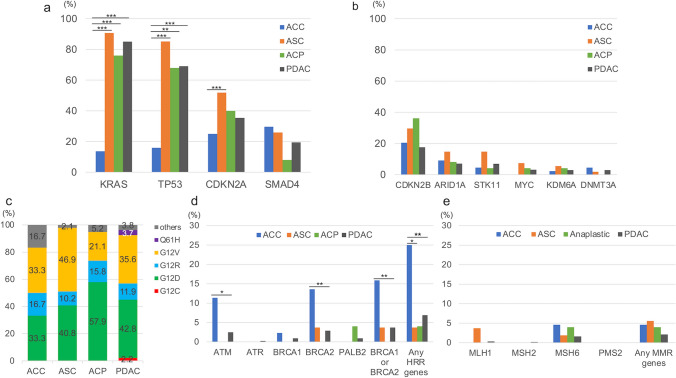
Results: Numbers of patients with ACC, ASC, ACP, and PDAC were 44 (1.6%), 54 (2.0%), 25 (0.9%), and 2,568 (95.4%), respectively. KRAS and TP53 mutations were prevalent in ASC, ACP, and PDAC (90.7/85.2, 76.0/68.0, and 85.1/69.1%, respectively), while their rates were both significantly lower in ACC (13.6/15.9%, respectively). Conversely, the rate of homologous recombination-related (HRR) genes, including ATM and BRCA1/2, was significantly higher in ACC (11.4/15.9%) than PDAC (2.5/3.7%). In ASC and ACP, no significant differences in ORR, DCR, or TTF between FFX and GnP were noted, while ACC patients showed a trend toward higher ORR with FFX than GnP (61.5 vs. 23.5%, p = 0.06) and significantly more favorable TTF (median 42.3 vs. 21.0 weeks, respectively, p = 0.004).
Conclusions: ACC clearly harbors different genomics compared with PDAC, possibly accounting for differences in treatment efficacy.
Keywords: Acinar cell carcinoma; Adenosquamous carcinoma; Anaplastic carcinoma of the pancreas; Genome analysis; Pancreatic ductal adenocarcinoma.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures

Comment in
-
C-CAT's triumph in gastroenterology: the wisdom of cats is infinitely superior.J Gastroenterol. 2024 Feb;59(2):157-158. doi: 10.1007/s00535-023-02061-z. Epub 2023 Nov 30. J Gastroenterol. 2024. PMID: 38032378 No abstract available.
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
