

Deep learning based automatic detection algorithm for acute intracranial haemorrhage: a pivotal randomized clinical trial
- PMID: 37029272
- PMCID: PMC10082037
- DOI: 10.1038/s41746-023-00798-8
Deep learning based automatic detection algorithm for acute intracranial haemorrhage: a pivotal randomized clinical trial
Abstract
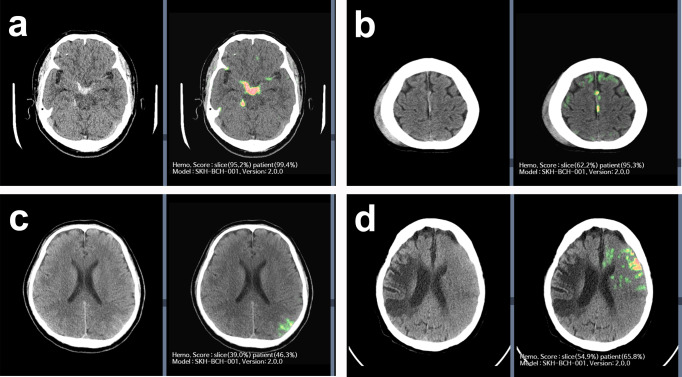
Acute intracranial haemorrhage (AIH) is a potentially life-threatening emergency that requires prompt and accurate assessment and management. This study aims to develop and validate an artificial intelligence (AI) algorithm for diagnosing AIH using brain-computed tomography (CT) images. A retrospective, multi-reader, pivotal, crossover, randomised study was performed to validate the performance of an AI algorithm was trained using 104,666 slices from 3010 patients. Brain CT images (12,663 slices from 296 patients) were evaluated by nine reviewers belonging to one of the three subgroups (non-radiologist physicians, n = 3; board-certified radiologists, n = 3; and neuroradiologists, n = 3) with and without the aid of our AI algorithm. Sensitivity, specificity, and accuracy were compared between AI-unassisted and AI-assisted interpretations using the chi-square test. Brain CT interpretation with AI assistance results in significantly higher diagnostic accuracy than that without AI assistance (0.9703 vs. 0.9471, p < 0.0001, patient-wise). Among the three subgroups of reviewers, non-radiologist physicians demonstrate the greatest improvement in diagnostic accuracy for brain CT interpretation with AI assistance compared to that without AI assistance. For board-certified radiologists, the diagnostic accuracy for brain CT interpretation is significantly higher with AI assistance than without AI assistance. For neuroradiologists, although brain CT interpretation with AI assistance results in a trend for higher diagnostic accuracy compared to that without AI assistance, the difference does not reach statistical significance. For the detection of AIH, brain CT interpretation with AI assistance results in better diagnostic performance than that without AI assistance, with the most significant improvement observed for non-radiologist physicians.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures




References
-
- Broderick J, et al. Guidelines for the management of spontaneous intracerebral hemorrhage in adults: 2007 update: a guideline from the American Heart Association/American Stroke Association Stroke Council, High Blood Pressure Research Council, and the Quality of Care and Outcomes in Research Interdisciplinary Working Group. Stroke. 2007;38:2001–2023. doi: 10.1161/STROKEAHA.107.183689. - DOI - PubMed
LinkOut - more resources
Full Text Sources
