

Simplifying minimally invasive right hepatectomy
- PMID: 37029324
- PMCID: PMC10322967
- DOI: 10.1007/s00464-023-09996-7
Simplifying minimally invasive right hepatectomy
Abstract
Background: Extrahepatic transection of the right hepatic artery and right portal vein before parenchymal dissection is a widely used standard for minimal invasive right hepatectomy. Hereby, hilar dissection represents a technical difficulty. We report our results of a simplified approach in which the hilar dissection is omitted and the line of dissection is defined with ultrasound.
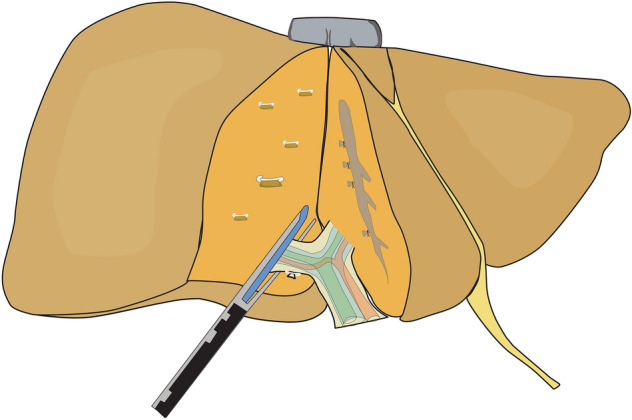
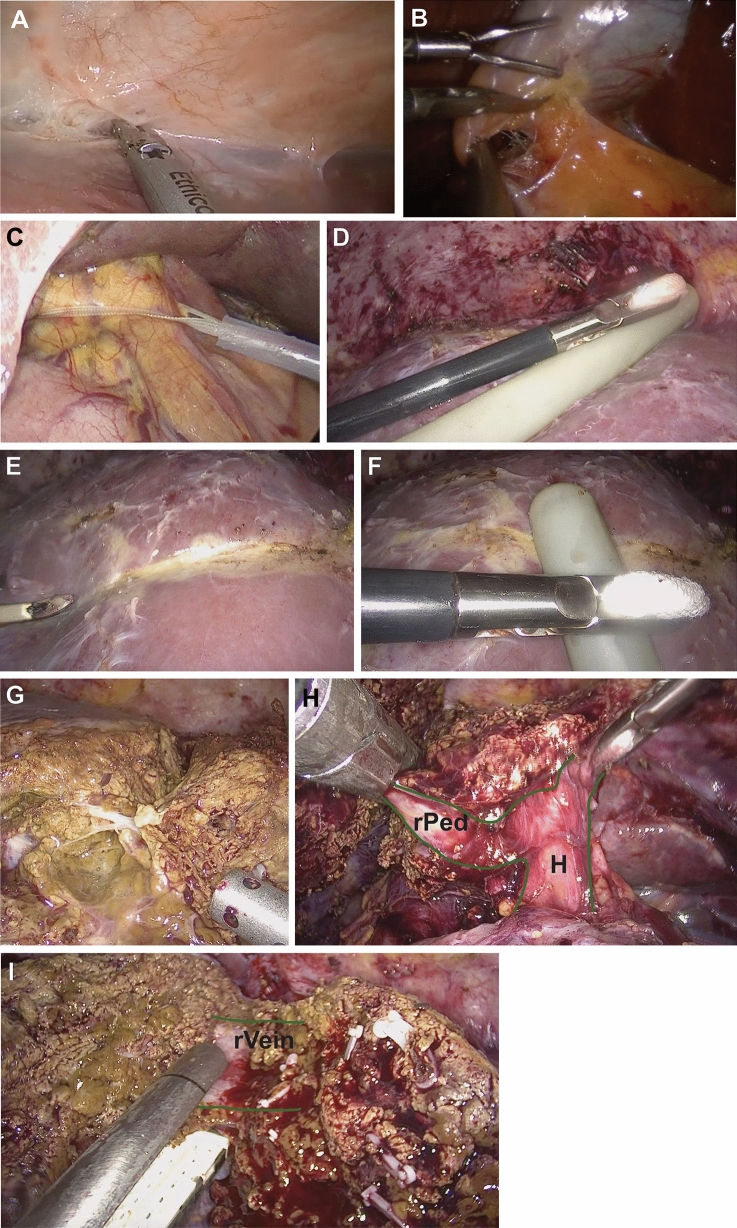
Methods: Patients undergoing minimally invasive right hepatectomy were included. Ultrasound-guided hepatectomy (UGH) was defined by the following main steps: (1) ultrasound-guided definition of the transection line, (2) dissection of the liver parenchyma according to the caudal approach, (3) intraparenchymal transection of the right pedicle and (4) of the right liver vein, respectively. Intra- and postoperative outcomes of UGH were compared to the standard technique. Propensity score matching was performed to adjust for parameters of perioperative risk.
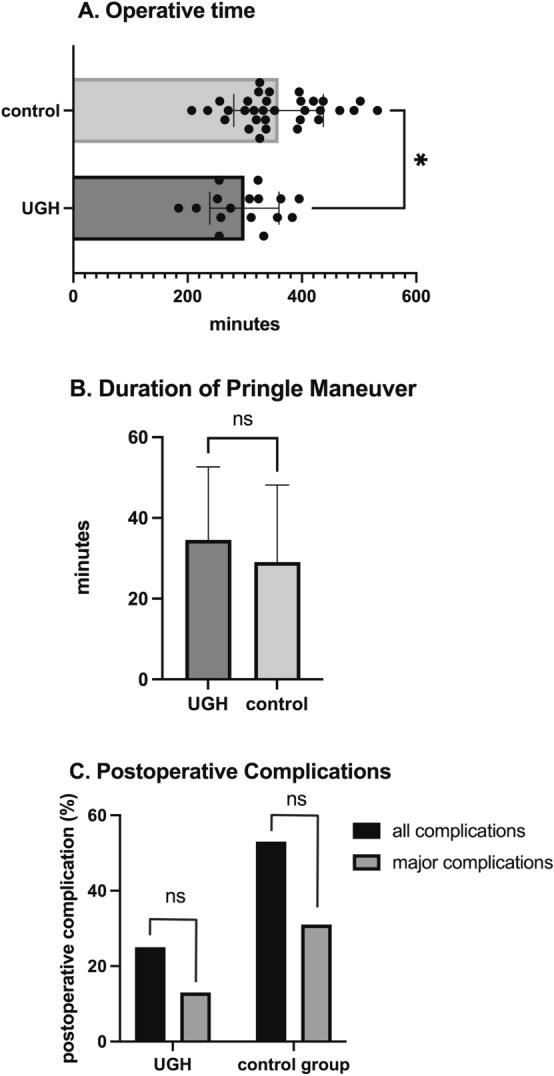
Results: Median operative time was 310 min in the UGH group compared to 338 min in the control group (p = 0.013). No differences were observed for Pringle maneuver duration (35 min vs. 25 min; p = ns) nor postoperative transaminases levels (p = ns). There was a trend toward a lower major complication rate in the UGH group (13 vs. 25%) and a shorter median hospital stay (8 days vs. 10 days); however, both being short of statistical significance (p = ns). Bile leak was observed in zero cases of UGH compared to 9 out of 32 cases (28%) for the control group (p = 0.020).
Conclusions: UGH appears to be at least comparable to the standard technique in terms of intraoperative and postoperative outcomes. Accordingly, transection of the right hepatic artery and right portal vein prior to the transection phase can be omitted, at least in selected cases. These results need to be confirmed in a prospective and randomized trial.
Keywords: Glissonean approach; Hepatectomy; Laparoscopic liver surgery; Robotic liver surgery.
© 2023. The Author(s).
Conflict of interest statement
Professor JP: received a research grant from Intuitive Surgical Deutschland GmbH for the conduction of the present study. Furthermore, he reports personal fees or other support from Johnson & Johnson, Medtronic, Astellas, CHG Meridian, AFS Medical, Chiesi, Falk Foundation, Neovii, NOGGO, pharma-consult Peterson, La Fource Group, Merck and promedicis. Professor MS: reports personal fees or non-financial support outside of the submitted work from Merck Serono GmbH, Bayer AG, ERBE Elektromedizin GmbH, Amgen Inc., Johnson&Johnson Medical GmbH, ERBE Elektromedizin GmbH, Takeda Pharmaceutical Limited, Olympus K.K., Medtronic GmbH, Intuitive Surgical Inc. Drs. NN, LF, SK, FK, NR, GL and Professor WS have no conflicts of interest or financial ties to disclose.
Figures
References
-
- Couinaud CM. A simplified method for controlled left hepatectomy. Surgery. 1985;97:358–361. - PubMed
-
- Takasaki K, Kobayashi S, Tanaka S, Saito A, Yamamoto M, Hanyu F. Highly anatomically systematized hepatic resection with Glissonean sheath code transection at the hepatic hilus. Int Surg. 1990;75:73–77. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
