

Diagnostic accuracy of clinical examination to identify life- and limb-threatening injuries in trauma patients
- PMID: 37029436
- PMCID: PMC10082501
- DOI: 10.1186/s13049-023-01083-z
Diagnostic accuracy of clinical examination to identify life- and limb-threatening injuries in trauma patients
Abstract
Background: Timely and accurate identification of life- and limb-threatening injuries (LLTIs) is a fundamental objective of trauma care that directly informs triage and treatment decisions. However, the diagnostic accuracy of clinical examination to detect LLTIs is largely unknown, due to the risk of contamination from in-hospital diagnostics in existing studies. Our aim was to assess the diagnostic accuracy of initial clinical examination for detecting life- and limb-threatening injuries (LLTIs). Secondary aims were to identify factors associated with missed injury and overdiagnosis, and determine the impact of clinician uncertainty on diagnostic accuracy.
Methods: Retrospective diagnostic accuracy study of consecutive adult (≥ 16 years) patients examined at the scene of injury by experienced trauma clinicians, and admitted to a Major Trauma Center between 01/01/2019 and 31/12/2020. Diagnoses of LLTIs made on contemporaneous clinical records were compared to hospital coded diagnoses. Diagnostic performance measures were calculated overall, and based on clinician uncertainty. Multivariate logistic regression analyses identified factors affecting missed injury and overdiagnosis.
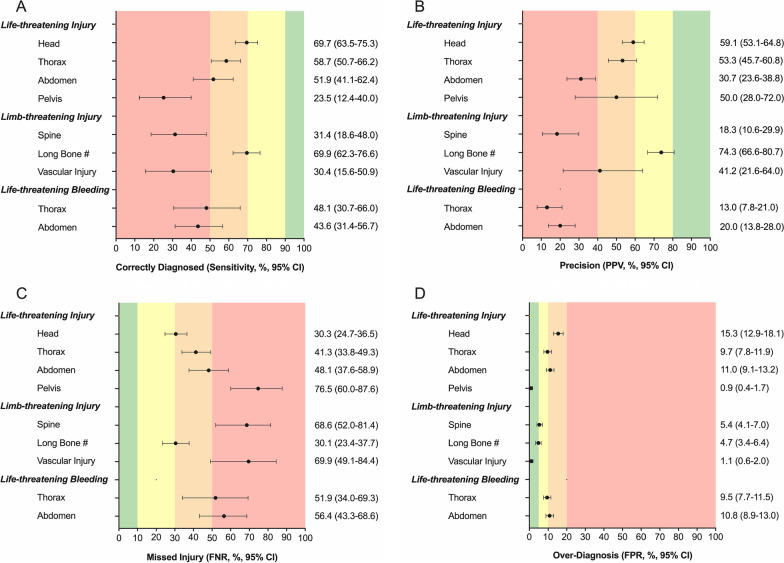
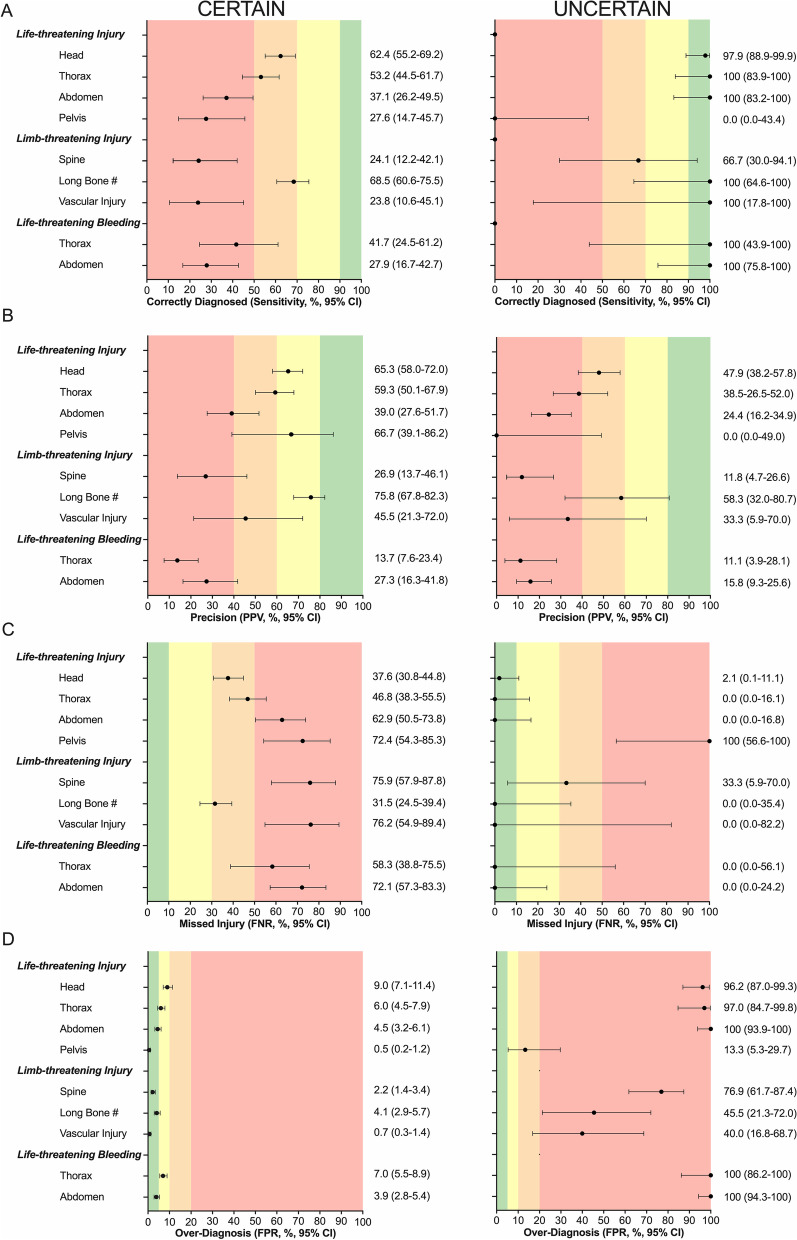
Results: Among 947 trauma patients, 821 were male (86.7%), median age was 31 years (range 16-89), 569 suffered blunt mechanisms (60.1%), and 522 (55.1%) sustained LLTIs. Overall, clinical examination had a moderate ability to detect LLTIs, which varied by body region: head (sensitivity 69.7%, positive predictive value (PPV) 59.1%), chest (sensitivity 58.7%, PPV 53.3%), abdomen (sensitivity 51.9%, PPV 30.7%), pelvis (sensitivity 23.5%, PPV 50.0%), and long bone fracture (sensitivity 69.9%, PPV 74.3%). Clinical examination poorly detected life-threatening thoracic (sensitivity 48.1%, PPV 13.0%) and abdominal (sensitivity 43.6%, PPV 20.0%) bleeding. Missed injury was more common in patients with polytrauma (OR 1.83, 95% CI 1.62-2.07) or shock (systolic blood pressure OR 0.993, 95% CI 0.988-0.998). Overdiagnosis was more common in shock (OR 0.991, 95% CI 0.986-0.995) or when clinicians were uncertain (OR 6.42, 95% CI 4.63-8.99). Uncertainty improved sensitivity but reduced PPV, impeding diagnostic precision.
Conclusions: Clinical examination performed by experienced trauma clinicians has only a moderate ability to detect LLTIs. Clinicians must appreciate the limitations of clinical examination, and the impact of uncertainty, when making clinical decisions in trauma. This study provides impetus for diagnostic adjuncts and decision support systems in trauma.
Keywords: Clinical examination; Diagnostic accuracy; Pre-hospital diagnosis; Traumatic injuries; Uncertainty.
© 2023. The Author(s).
Conflict of interest statement
JMW received funding from the Royal College of Surgeons of England for salary support during the conduct of the study. RSS received funding from the Royal College of Surgeons of Edinburgh for salary support during the conduct of the study. The other authors declare that they have no competing interests.
Figures


References
-
- Lockey D, Deakin CD. Pre-hospital trauma care: systems and delivery. Contin Educ Anaesthesia Crit Care Pain. 2005;5(6):191–194. doi: 10.1093/bjaceaccp/mki054. - DOI
-
- American College of Surgeons Committee on T. Advanced Trauma Life Support: tenth edition. tenth ed. Chicago, IL: American College of Surgeons; 2018.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
