

Chronic Airways Assessment Test: psychometric properties in patients with asthma and/or COPD
- PMID: 37031164
- PMCID: PMC10082977
- DOI: 10.1186/s12931-023-02394-6
Chronic Airways Assessment Test: psychometric properties in patients with asthma and/or COPD
Abstract
Background: No short patient-reported outcome (PRO) instruments assess overall health status across different obstructive lung diseases. Thus, the wording of the introduction to the Chronic Obstructive Pulmonary Disease (COPD) Assessment Test (CAT) was modified to permit use in asthma and/or COPD. This tool is called the Chronic Airways Assessment Test (CAAT).
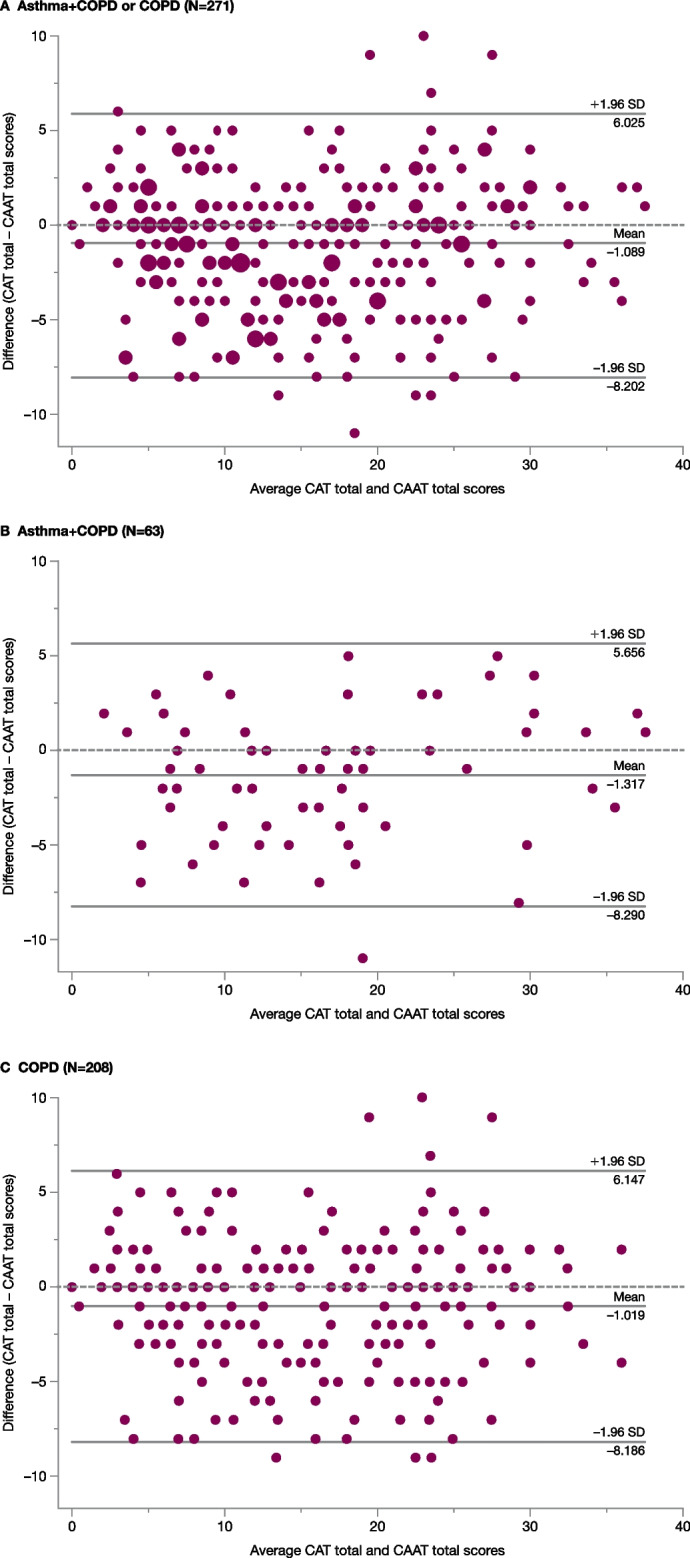
Methods: The psychometric properties of the CAAT were evaluated using baseline data from the NOVELTY study (NCT02760329) in patients with physician-assigned asthma, asthma + COPD or COPD. Analyses included exploratory/confirmatory factor analyses, differential item functioning and analysis of construct validity. Responses to the CAAT and CAT were compared in patients with asthma + COPD and those with COPD.
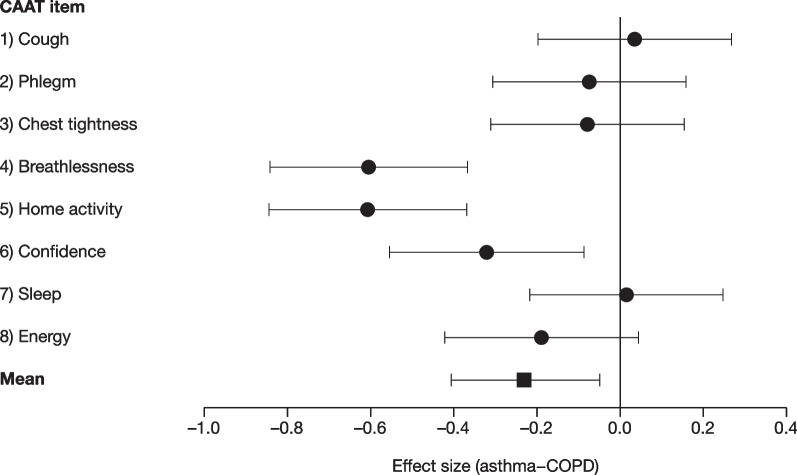
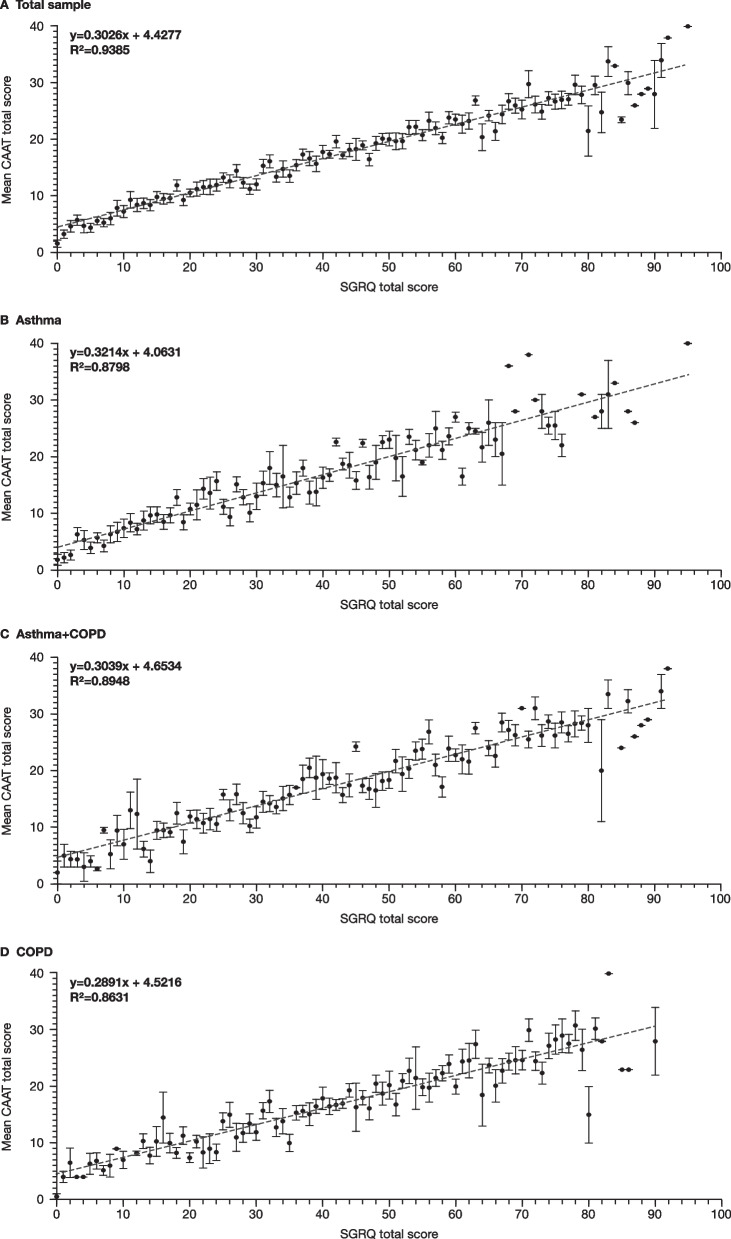
Results: CAAT items were internally consistent (Cronbach's alpha: > 0.7) within each diagnostic group (n = 510). Models for structural and measurement invariance were strong. Tests of differential item functioning showed small differences between asthma and COPD in individual items, but these were not consistent in direction and had minimal overall impact on the total score. The CAAT and CAT were highly consistent when assessed in all NOVELTY patients who completed both (N = 277, Pearson's correlation coefficient: 0.90). Like the CAT itself, CAAT scores correlated moderately (0.4-0.7) to strongly (> 0.7) with other PRO measures and weakly (< 0.4) with spirometry measures.
Conclusions: CAAT scores appear to reflect the same health impairment across asthma and COPD, making the CAAT an appropriate PRO instrument for patients with asthma and/or COPD. Its brevity makes it suitable for use in clinical studies and routine clinical practice.
Trial registration: NCT02760329.
Keywords: Asthma; COPD; COPD Assessment Test; Chronic Airways Assessment Test; Patient-reported; Psychometrics.
© 2023. The Author(s).
Conflict of interest statement
ELT, NK and HM are employees of AstraZeneca. MJA reports payment as an independent consultant to Evidera Inc. for activities contracted by AstraZeneca in relation to the psychometric evaluation of the CAAT; he has provided analytic direction and unbiased interpretation of the CAAT findings. CJ reports personal fees from AstraZeneca, Boehringer Ingelheim, Chiesi, GlaxoSmithKline, Novartis and Teva Pharmaceuticals. PWJ is an employee of GlaxoSmithKline and owns GlaxoSmithKline stocks and shares. BM reports grants (with funds provided to, and controlled by, National Jewish Health) from AstraZeneca, GlaxoSmithKline, NIH National Heart, Lung, and Blood Institute, Pearl Research and Sunovion; personal fees from Takeda and Third Pole; non-financial support from AstraZeneca, Circassia, GlaxoSmithKline, Phillips, Shire, Spiration, Sunovion and Third Pole; and other from Academy Continued Health Care Learning, American College of Chest Physicians, AstraZeneca, Boehringer Ingelheim, Catamount Medical, Circassia, Eastern Pulmonary Society, Eastern VA Medical Center, GlaxoSmithKline, Hybrid Communications, Medscape, Mount Sinai Medical Center, National Jewish Health, Novartis, Phillips, Projects in Knowledge, Science 24/7, Shire, Sunovion, Theravance, Ultimate Medical Academy, Verona, WebMD and Wolters Kluwer Health. DP reports funding for the conduct of this study from AstraZeneca, and discloses board membership with Amgen, AstraZeneca, Boehringer Ingelheim, Chiesi, Circassia, Mundipharma, Mylan, Novartis, Regeneron Pharmaceuticals, Sanofi Genzyme, Teva Pharmaceuticals and Thermo Fisher Scientific; consultancy fees from Amgen, AstraZeneca, Boehringer Ingelheim, Chiesi, GlaxoSmithKline, Mundipharma, Mylan, Novartis, Pfizer, Teva Pharmaceuticals and Theravance; grants and unrestricted funding for investigator-initiated studies (conducted through Observational and Pragmatic Research Institute Pte Ltd) from AstraZeneca, Boehringer Ingelheim, Chiesi, Circassia, Mundipharma, Mylan, Novartis, Pfizer, Regeneron Pharmaceuticals, Respiratory Effectiveness Group, Sanofi Genzyme, Teva Pharmaceuticals, Theravance and the UK National Health Service; lecture/speaking engagement fees from AstraZeneca, Boehringer Ingelheim, Chiesi, Cipla, GlaxoSmithKline, Kyorin, Mundipharma, Mylan, Novartis, Regeneron Pharmaceuticals, Sanofi Genzyme and Teva Pharmaceuticals; payment for the development of educational materials from Mundipharma and Novartis; travel/accommodation/meeting expenses from AstraZeneca, Boehringer Ingelheim, Mundipharma, Mylan, Novartis and Thermo Fisher Scientific; funding for patient enrolment or completion of research from Novartis; stock/stock options from AKL Research and Development Ltd, which produces phytopharmaceuticals; owns 74% of the social enterprise Optimum Patient Care Ltd (Australia and UK) and 74% of Observational and Pragmatic Research Institute Pte Ltd (Singapore); 5% shareholding in Timestamp, which develops adherence monitoring technology; is peer reviewer for grant committees of the Efficacy and Mechanism Evaluation programme and Health Technology Assessment; and was an expert witness for GlaxoSmithKline. HKR has participated in advisory boards for AstraZeneca, Chiesi, GlaxoSmithKline, Novartis and Sanofi Genzyme; and has received honoraria from AstraZeneca, Boehringer Ingelheim, Chiesi, GlaxoSmithKline, Sanofi and Teva Pharmaceuticals for independent medical educational presentations; consulting for Novartis and AstraZeneca; and independent research funding from AstraZeneca, GlaxoSmithKline and Novartis. She is Chair of the Global Institute for Asthma Science Committee and a member of the Australian National Asthma Council Guidelines Committee. CFV has given presentations at symposia and/or served on scientific advisory boards sponsored by AstraZeneca, Boehringer Ingelheim, Chiesi, CSL Behring, GlaxoSmithKline, Grifols, MedUpdate, Menarini, Novartis and Nuvaira.
Figures
References
-
- US Food and Drug Administration. Guidance for Industry. Patient-reported outcome measures: use in medical product development to support labeling claims. 2009. https://www.fda.gov/media/77832/download. Accessed 22 Apr 2022.
-
- US Food and Drug Administration. Chronic obstructive pulmonary disease: use of the St. George’s Respiratory Questionnaire as a PRO assessment tool. Guidance for industry. 2018. https://www.fda.gov/files/drugs/published/Chronic-Obstructive-Pulmonary-.... Accessed 22 Apr 2022.
-
- European Medicines Agency. Reflection paper on the regulatory guidance for the use of health-related quality of life (HRQL) measures in the evaluation of medicinal products. 2005. https://www.ema.europa.eu/en/documents/scientific-guideline/reflection-p.... Accessed 22 Apr 2022.
