

The increase in cardiac output induced by a decrease in positive end-expiratory pressure reliably detects volume responsiveness: the PEEP-test study
- PMID: 37031182
- PMCID: PMC10082988
- DOI: 10.1186/s13054-023-04424-7
The increase in cardiac output induced by a decrease in positive end-expiratory pressure reliably detects volume responsiveness: the PEEP-test study
Abstract
Background: In patients on mechanical ventilation, positive end-expiratory pressure (PEEP) can decrease cardiac output through a decrease in cardiac preload and/or an increase in right ventricular afterload. Increase in central blood volume by fluid administration or passive leg raising (PLR) may reverse these phenomena through an increase in cardiac preload and/or a reopening of closed lung microvessels. We hypothesized that a transient decrease in PEEP (PEEP-test) may be used as a test to detect volume responsiveness.
Methods: Mechanically ventilated patients with PEEP ≥ 10 cmH2O ("high level") and without spontaneous breathing were prospectively included. Volume responsiveness was assessed by a positive PLR-test, defined as an increase in pulse-contour-derived cardiac index (CI) during PLR ≥ 10%. The PEEP-test consisted in reducing PEEP from the high level to 5 cmH2O for one minute. Pulse-contour-derived CI (PiCCO2) was monitored during PLR and the PEEP-test.
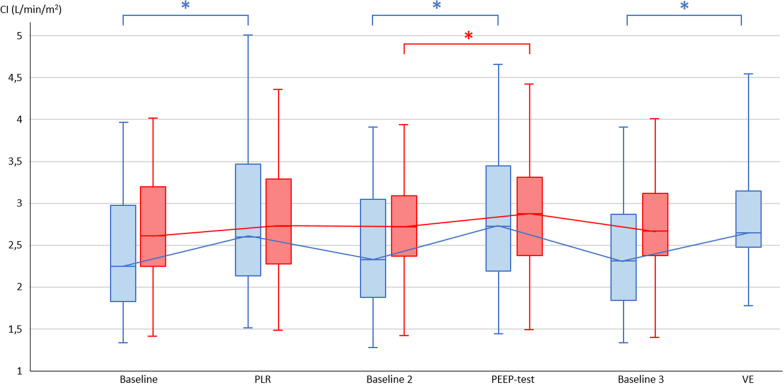
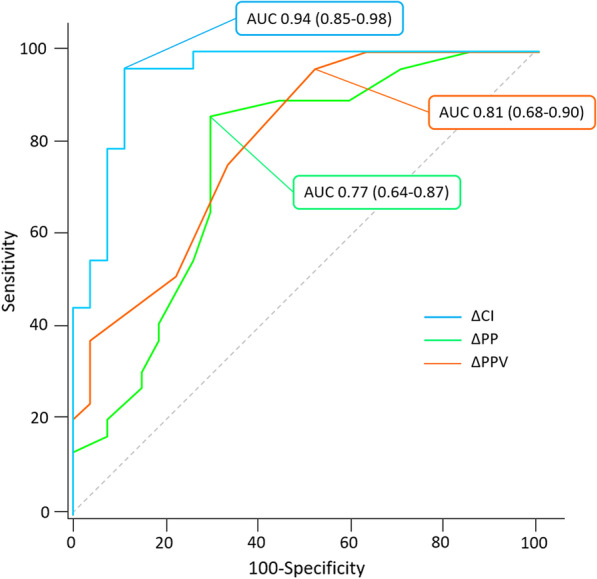
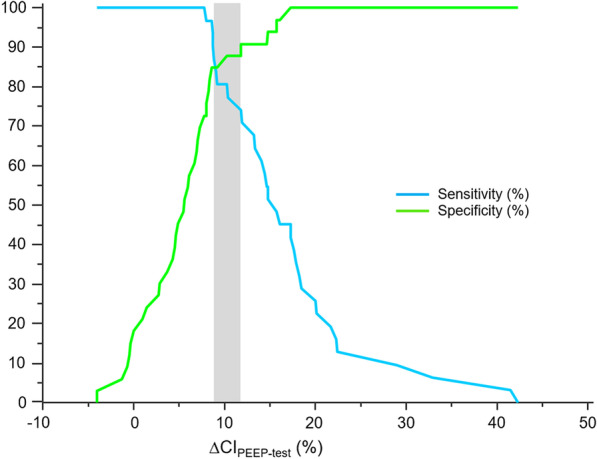
Results: We enrolled 64 patients among whom 31 were volume responsive. The median increase in CI during PLR was 14% (11-16%). The median PEEP at baseline was 12 (10-15) cmH2O and the PEEP-test resulted in a median decrease in PEEP of 7 (5-10) cmH2O, without difference between volume responsive and unresponsive patients. Among volume responsive patients, the PEEP-test induced a significant increase in CI of 16% (12-20%) (from 2.4 ± 0.7 to 2.9 ± 0.9 L/min/m2, p < 0.0001) in comparison with volume unresponsive patients. In volume unresponsive patients, PLR and the PEEP-test increased CI by 2% (1-5%) and 6% (3-8%), respectively. Volume responsiveness was predicted by an increase in CI > 8.6% during the PEEP-test with a sensitivity of 96.8% (95% confidence interval (95%CI): 83.3-99.9%) and a specificity of 84.9% (95%CI 68.1-94.9%). The area under the receiver operating characteristic curve of the PEEP-test for detecting volume responsiveness was 0.94 (95%CI 0.85-0.98) (p < 0.0001 vs. 0.5). Spearman's correlation coefficient between the changes in CI induced by PLR and the PEEP-test was 0.76 (95%CI 0.63-0.85, p < 0.0001).
Conclusions: A CI increase > 8.6% during a PEEP-test, which consists in reducing PEEP to 5 cmH2O, reliably detects volume responsiveness in mechanically ventilated patients with a PEEP ≥ 10 cmH2O. Trial registration ClinicalTrial.gov (NCT 04,023,786). Registered July 18, 2019. Ethics Committee approval CPP Est III (N° 2018-A01599-46).
Keywords: ARDS; Fluid responsiveness; Hemodynamic monitoring; Passive leg raising; Shock.
© 2023. The Author(s).
Conflict of interest statement
C.L. received honoraria for lectures from Sedana Medical. X.M. is a member of the Medical Advisory Board of Pulsion Medical Systems (Getinge) and received honoraria for lectures from Pulsion Medical Systems (Getinge) and Baxter. J-L.T. is a member of the Medical Advisory Board of Pulsion Medical Systems (Getinge).
Figures
Comment in
-
Can fluid responsiveness tests utilizing positive end-expiratory pressure changes be adapted to improve applicability in all mechanically ventilated patients?Crit Care. 2023 May 17;27(1):191. doi: 10.1186/s13054-023-04483-w. Crit Care. 2023. PMID: 37198634 Free PMC article. No abstract available.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
