A multicenter evaluation of a deep learning software (LungQuant) for lung parenchyma characterization in COVID-19 pneumonia
- PMID: 37032383
- PMCID: PMC10083148
- DOI: 10.1186/s41747-023-00334-z
A multicenter evaluation of a deep learning software (LungQuant) for lung parenchyma characterization in COVID-19 pneumonia
Abstract
Background: The role of computed tomography (CT) in the diagnosis and characterization of coronavirus disease 2019 (COVID-19) pneumonia has been widely recognized. We evaluated the performance of a software for quantitative analysis of chest CT, the LungQuant system, by comparing its results with independent visual evaluations by a group of 14 clinical experts. The aim of this work is to evaluate the ability of the automated tool to extract quantitative information from lung CT, relevant for the design of a diagnosis support model.
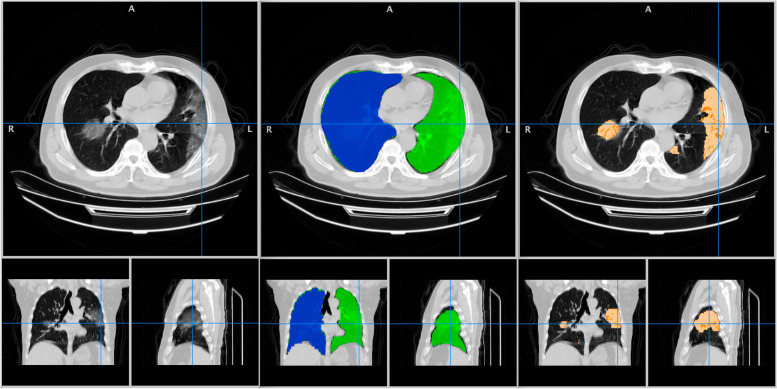
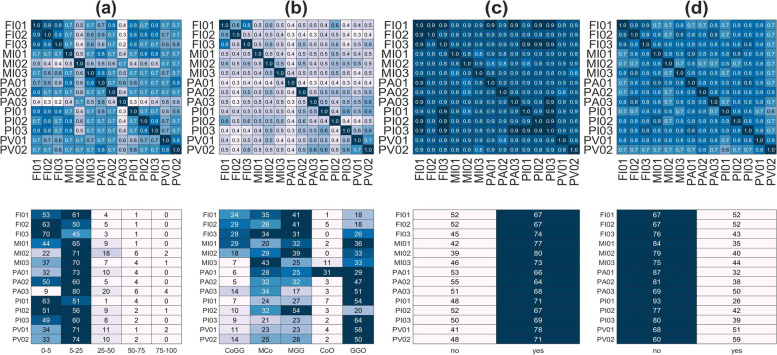
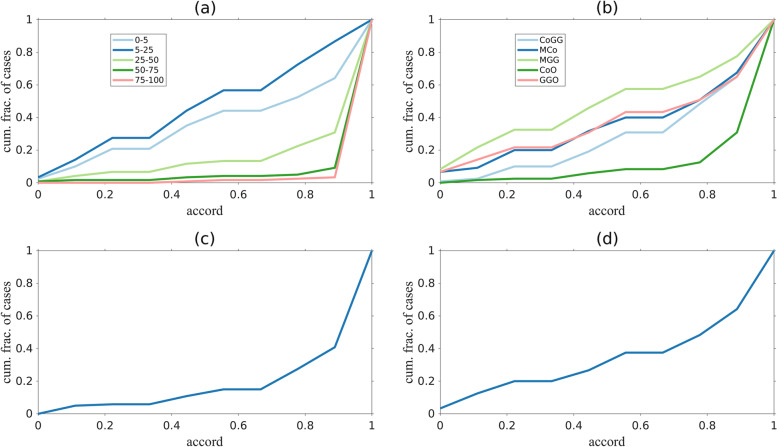
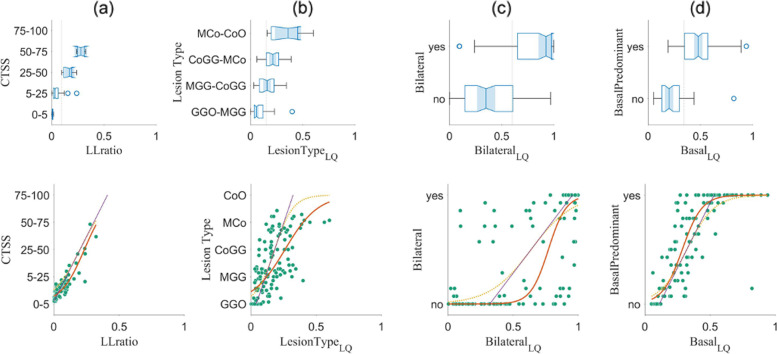
Methods: LungQuant segments both the lungs and lesions associated with COVID-19 pneumonia (ground-glass opacities and consolidations) and computes derived quantities corresponding to qualitative characteristics used to clinically assess COVID-19 lesions. The comparison was carried out on 120 publicly available CT scans of patients affected by COVID-19 pneumonia. Scans were scored for four qualitative metrics: percentage of lung involvement, type of lesion, and two disease distribution scores. We evaluated the agreement between the LungQuant output and the visual assessments through receiver operating characteristics area under the curve (AUC) analysis and by fitting a nonlinear regression model.
Results: Despite the rather large heterogeneity in the qualitative labels assigned by the clinical experts for each metric, we found good agreement on the metrics compared to the LungQuant output. The AUC values obtained for the four qualitative metrics were 0.98, 0.85, 0.90, and 0.81.
Conclusions: Visual clinical evaluation could be complemented and supported by computer-aided quantification, whose values match the average evaluation of several independent clinical experts.
Key points: We conducted a multicenter evaluation of the deep learning-based LungQuant automated software. We translated qualitative assessments into quantifiable metrics to characterize coronavirus disease 2019 (COVID-19) pneumonia lesions. Comparing the software output to the clinical evaluations, results were satisfactory despite heterogeneity of the clinical evaluations. An automatic quantification tool may contribute to improve the clinical workflow of COVID-19 pneumonia.
Keywords: COVID-19; Deep Learning; Lung; Software validation; Tomography (x-ray computed).
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Emanuele Neri is a member of the Scientific Editorial Board of the
Figures