

MRI hip morphology is abnormal in unilateral DDH and increased lateral limbus thickness is associated with residual DDH at minimum 10-year follow-up
- PMID: 37034197
- PMCID: PMC10080238
- DOI: 10.1177/18632521221144060
MRI hip morphology is abnormal in unilateral DDH and increased lateral limbus thickness is associated with residual DDH at minimum 10-year follow-up
Abstract
Purpose: The purpose of the study was to compare the post-reduction magnetic resonance imaging morphology for hips that developed residual acetabular dysplasia, hips without residual dysplasia, and uninvolved contralateral hips in patients with unilateral developmental dysplasia of the hip undergoing closed or open reduction and had a minimum 10-year follow-up.
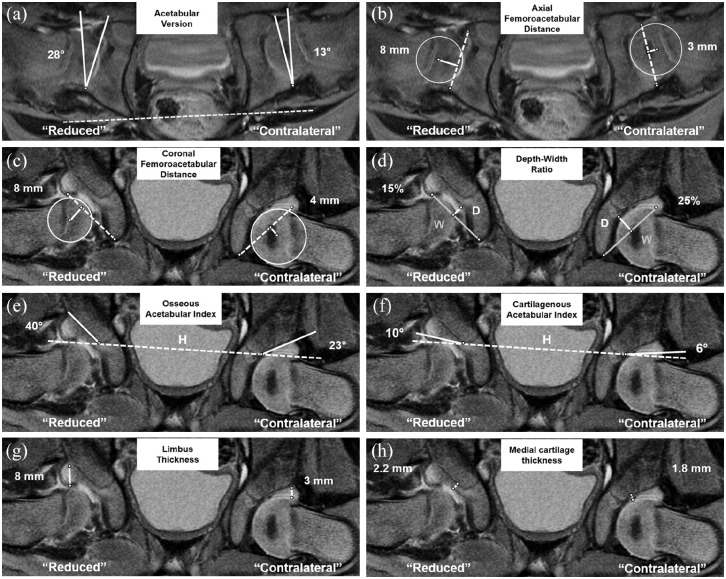
Methods: Retrospective study of patients with unilateral dysplasia of the hip who underwent open/closed hip reduction followed by post-reduction magnetic resonance imaging. Twenty-eight patients with a mean follow-up of 13 ± 3 years were included. In the treated hips, residual dysplasia was defined as subsequent surgery for residual acetabular dysplasia or for Severin grade > 2 at latest follow-up. On post-reduction, magnetic resonance imaging measurements were performed by two readers and compared between the hips with/without residual dysplasia and the contralateral uninvolved side. Magnetic resonance imaging measurements included acetabular version, coronal/ axial femoroacetabular distance, acetabular depth-width ratio, osseous/cartilaginous acetabular indices, and medial/lateral (limbus) cartilage thickness.
Results: Fifteen (54%) and 13 (46%) hips were allocated to the "no residual dysplasia" group and to the "residual dysplasia" group, respectively. All eight magnetic resonance imaging parameters differed between hips with residual dysplasia and contralateral uninvolved hips (all p < 0.05). Six of eight parameters differed (all p < 0.05) between hips with and without residual dysplasia. Among these, increased limbus thickness had the largest effect (odds ratio = 12.5; p < 0.001) for increased likelihood of residual dysplasia.
Conclusions: We identified acetabular morphology and reduction quality parameters that can be reliably measured on the post-reduction magnetic resonance imaging to facilitate the differentiation between hips that develop with/without residual acetabular dysplasia at 10 years postoperatively.
Level of evidence: level III, prognostic case-control study.
Keywords: Post-reduction MRI; developmental dysplasia of the hip; hip; hip MRI; surgical hip reduction.
© The Author(s) 2022.
Conflict of interest statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures

Similar articles
-
Hip Morphology on Post-Reduction MRI Predicts Residual Dysplasia 10 Years After Open or Closed Reduction.J Bone Joint Surg Am. 2024 Jan 17;106(2):110-119. doi: 10.2106/JBJS.23.00333. Epub 2023 Nov 22. J Bone Joint Surg Am. 2024. PMID: 37992184 Free PMC article.
-
Which Acetabular Landmarks are the Most Useful for Measuring the Acetabular Index and Center-edge Angle in Developmental Dysplasia of the Hip? A Comparison of Two Methods.Clin Orthop Relat Res. 2020 Sep;478(9):2120-2131. doi: 10.1097/CORR.0000000000001289. Clin Orthop Relat Res. 2020. PMID: 32379138 Free PMC article.
-
Prognosticating Residual Dysplasia at Skeletal Maturity Following Closed Reduction for Developmental Dysplasia of the Hip: A Long-Term Study with an Average 20-Year Follow-up.J Bone Joint Surg Am. 2024 Nov 20;106(22):2094-2101. doi: 10.2106/JBJS.23.01484. Epub 2024 Sep 18. J Bone Joint Surg Am. 2024. PMID: 39292809
-
MRI assessment of femoral head docking following closed reduction of developmental dysplasia of the hip.Bone Joint J. 2023 Feb;105-B(2):140-147. doi: 10.1302/0301-620X.105B2.BJJ-2022-0547.R2. Bone Joint J. 2023. PMID: 36722051 Free PMC article. Review.
-
Outcome Prognostic Factors in MRI during Spica Cast Therapy Treating Developmental Hip Dysplasia with Midterm Follow-Up.Children (Basel). 2022 Jul 7;9(7):1010. doi: 10.3390/children9071010. Children (Basel). 2022. PMID: 35883994 Free PMC article. Review.
Cited by
-
Predictive importance of cartilage acetabular index for acetabular dysplasia in orthopedic surgery.Acta Cir Bras. 2025 Jan 13;40:e400625. doi: 10.1590/acb400625. eCollection 2025. Acta Cir Bras. 2025. PMID: 39813533 Free PMC article.
-
Reg3β promotes chondrocyte proliferation and ECM metabolism during acetabular roof remodeling in a rat model of DDH‑induced residual dysplasia.Mol Med Rep. 2025 Nov;32(5):288. doi: 10.3892/mmr.2025.13653. Epub 2025 Aug 24. Mol Med Rep. 2025. PMID: 40849812 Free PMC article.
-
Hip Morphology on Post-Reduction MRI Predicts Residual Dysplasia 10 Years After Open or Closed Reduction.J Bone Joint Surg Am. 2024 Jan 17;106(2):110-119. doi: 10.2106/JBJS.23.00333. Epub 2023 Nov 22. J Bone Joint Surg Am. 2024. PMID: 37992184 Free PMC article.
References
-
- Weinstein SL, Mubarak SJ, Wenger DR. Developmental hip dysplasia and dislocation: part II. Instr Course Lect 2004; 53: 531–542. - PubMed
-
- Chin MS, Betz BW, Halanski MA. Comparison of hip reduction using magnetic resonance imaging or computed tomography in hip dysplasia. J Pediatr Orthop 2011; 31(5): 525–529. - PubMed
-
- Chin MS, Shoemaker A, Reinhart DM, et al.. Use of 1.5 Tesla and 3 Tesla MRI to evaluate femoral head reduction in hip dysplasia. J Pediatr Orthop 2011; 31(6): 633–637. - PubMed
-
- Dibello D, Odoni L, Pederiva F, et al.. MRI in postreduction evaluation of developmental dysplasia of the hip. J Pediatr Orthop 2019; 39(9): 449–452. - PubMed
-
- Duffy CM, Taylor FN, Coleman L, et al.. Magnetic resonance imaging evaluation of surgical management in developmental dysplasia of the hip in childhood. J Pediatr Orthop 2002; 22(1): 92–100. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials