

Is the duration of dual antiplatelet therapy (DAPT) excessive in post-angioplasty in chronic coronary syndrome? Data from the France-PCI registry (2014-2019)
- PMID: 37034332
- PMCID: PMC10080068
- DOI: 10.3389/fcvm.2023.1106503
Is the duration of dual antiplatelet therapy (DAPT) excessive in post-angioplasty in chronic coronary syndrome? Data from the France-PCI registry (2014-2019)
Abstract
Background: while the duration of dual antiplatelet therapy (DAPT) following coronary angioplasty for chronic coronary syndrome (CCS) recommended by the European Society of Cardiology has decreased over the last decade, little is known about the adherence to those guidelines in clinical practice in France.
Aim: To analyze the real duration of DAPT post coronary angioplasty in CCS, as well as the factors affecting this duration.
Methods: Between 2014 and 2019, 8.836 percutaneous coronary interventions for CCS from the France-PCI registry were evaluated, with 1 year follow up, after exclusion of patients receiving oral anticoagulants, procedures performed within one year of an acute coronary syndrome, and repeat angioplasty.
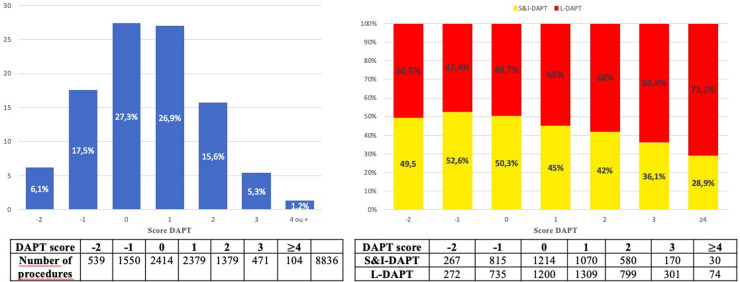
Results: Post-percutaneous coronary intervention (PCI) DAPT duration was > 12 months for 53.1% of patients treated for CCS; 30.5% had a DAPT between 7 and 12 months, and 16.4% a DAPT ≤ 6 months. Patients with L-DAPT (>12 months) were at higher ischemic risk [25.0% of DAPT score ≥2 vs. 18.8% DAPT score ≥2 in S&I-DAPT group (≤12 months)]. The most commonly used P2Y12 inhibitor was clopidogrel (82.2%). The prescription of ticagrelor increased over the period.
Conclusions: post-PCI DAPT duration in CCS was higher than international recommendations in the France PCI registry between 2014 and 2019. More than half of the angioplasty performed for CCS are followed by a DAPT > 12 months. Ischemic risk assessment influences the duration of DAPT. This risk is probably overestimated nowadays, leading to a prolongation of DAPT beyond the recommended durations, thus increasing the bleeding risk.
Keywords: bleeding risk; chronic coronary syndrome; coronary angioplasty; dual antiplatelet therapy; ischemic risk.
© 2023 Mezier, Motreff, Clerc, Bar, Deballon, Demicheli, Dechery, Souteyrand, Py, Lhoest, Lhermusier, Honton, Gommeaux, Jeanneteau, Deharo, Benamer, Cayla, Koning, Pereira, Collet and Rangé.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures



References
-
- Machado C, Raposo L, Dores H, Leal S, Campante Teles R, de Araújo Gonçalves P, et al. Second-generation versus first-generation drug-eluting stents for the treatment of patients with acute coronary syndromes and obstructive coronary artery disease. Coron Artery Dis. (2014) 25(3):208–14. 10.1097/MCA.0000000000000078 - DOI - PubMed
-
- Valgimigli M, Bueno H, Byrne RA, Collet JP, Costa F, Jeppsson A, et al. 2017 ESC focused update on dual antiplatelet therapy in coronary artery disease developed in collaboration with EACTS: the task force for dual antiplatelet therapy in coronary artery disease of the European society of cardiology (ESC) and of the European association for cardio-thoracic surgery (EACTS). Eur Heart J. (2018) 39(3):213–60. 10.1093/eurheartj/ehx419 - DOI - PubMed
-
- Montalescot G, Sechtem U, Achenbach S, Andreotti F, Arden C, Budaj A, et al. 2013 ESC guidelines on the management of stable coronary artery disease: the task force on the management of stable coronary artery disease of the European society of cardiology. Eur Heart J. (2013) 34(38):2949–3003. 10.1093/eurheartj/eht296 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous