

Cigarette Smoking, and Blood Monocyte Count Correlate with Chronic Lung Injuries and Mortality
- PMID: 37034898
- PMCID: PMC10076620
- DOI: 10.2147/COPD.S397667
Cigarette Smoking, and Blood Monocyte Count Correlate with Chronic Lung Injuries and Mortality
Abstract
Background: Cigarette smoking (CS)-related monocytosis contributes to the development of chronic lung injuries via complex mechanisms. We aim to determine correlations between measures of CS and monocytes, their capacities to predict chronic lung diseases, and their associations with mortality.
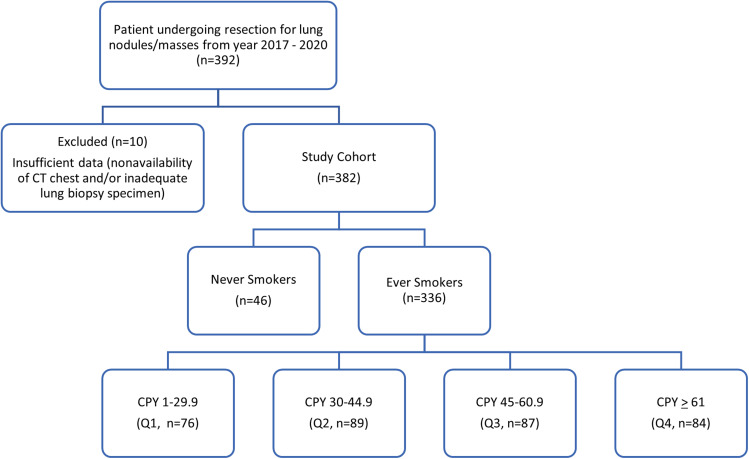
Methods: A single-center retrospective study of patients undergoing surgical resection for suspected lung nodules/masses was performed. CS was quantified as cigarettes smoked per day (CPD), duration of smoking, composite pack years (CPY), current smoking status, and smoking cessation years. A multivariate logistic regression analysis was performed.
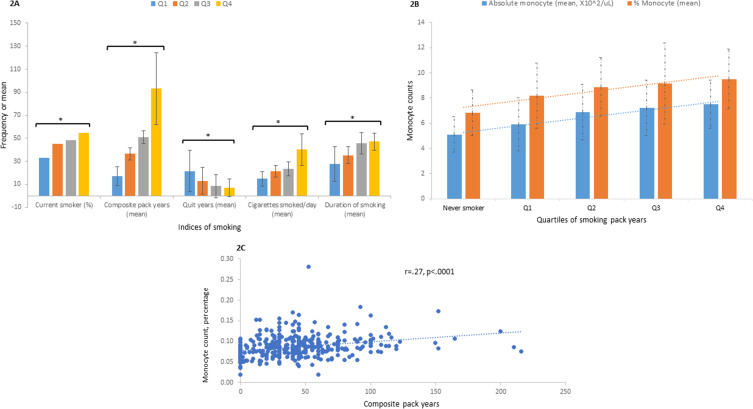
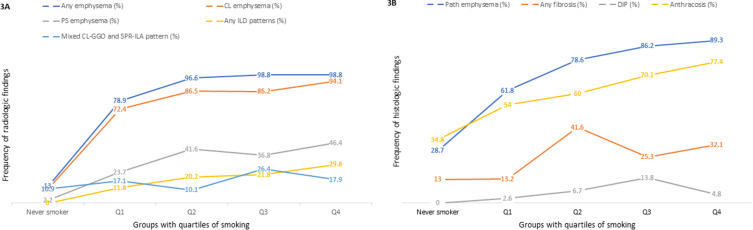
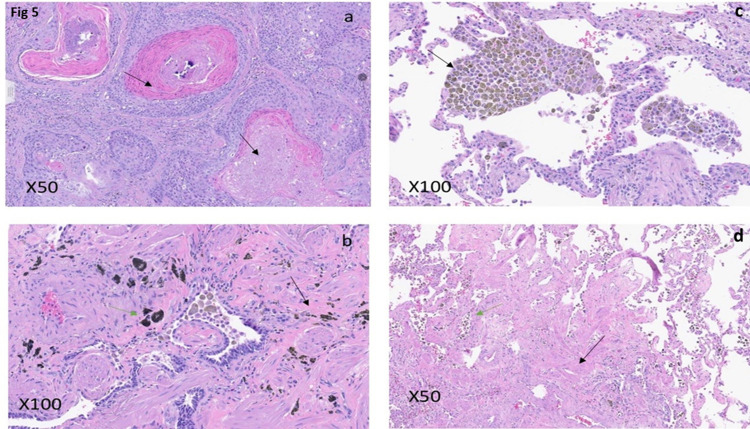
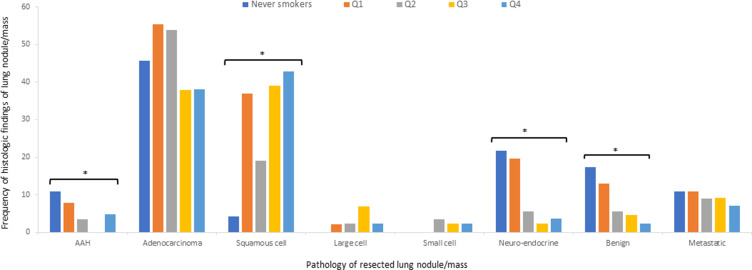
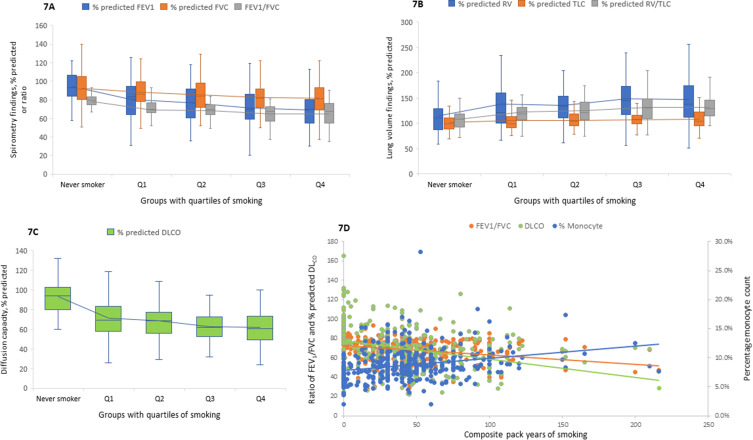
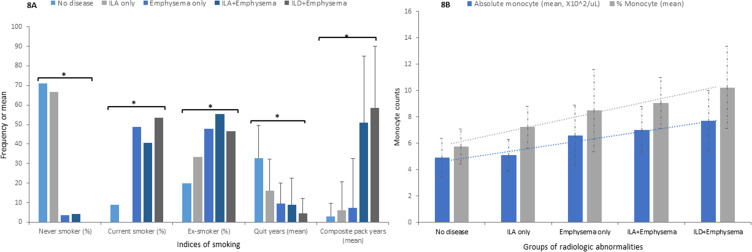
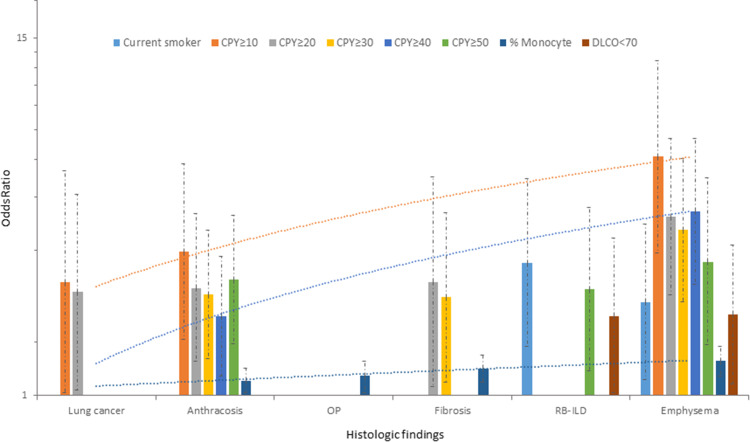
Results: Of 382 eligible patients, 88% were ever smokers. In this group, 45% were current smokers with mean CPD of 27.2±40.0. CPY and duration of smoking showed positive linear correlations with percentage monocyte count. Physiologically, CPY was associated with progressive obstruction, hyperinflation, and reduced diffusion capacity (DLCO). Across the quartiles of smoking, there was an accumulation of radiologic and histologic abnormalities. Anthracosis and emphysema were associated with CPD, while lung cancer, respiratory bronchiolitis (RB), emphysema, and honeycombing were statistically related to duration of smoking. Analysis using consecutive CPY showed associations with lung cancer (≥10 and <30), fibrosis (≥20 and <40), RB (≥50), anthracosis and emphysema (≥10 and onwards). Percentage monocytes correlated with organizing pneumonia (OP), fibrosis, and emphysema. The greater CPY increased mortality across the groups. Significant predictors of mortality included percentage monocyte, anemia, GERD, and reduced DLCO.
Conclusion: Indices of CS and greater monocyte numbers were associated with endpoints of chronic lung disease suggesting a participation in pathogenesis. Application of these easily available metrics may support a chronology of CS-induced chronic lung injuries. While a relative lesser amount of smoking can be associated with lung cancer and fibrosis, greater CPY increases the risk for emphysema. Monocytosis predicted lung fibrosis and mortality. Duration of smoking may serve as a better marker of monocytosis and associated chronic lung diseases.
Keywords: emphysema; lung cancer; monocyte; mortality; pulmonary fibrosis; smoking.
© 2023 Sangani et al.
Conflict of interest statement
The authors declare they have no financial or non-financial competing interests in this work.
Figures
Similar articles
-
Impact of coal mine dust exposure and cigarette smoking on lung disease in Appalachian coalminers.Respir Res. 2025 May 14;26(1):184. doi: 10.1186/s12931-025-03260-3. Respir Res. 2025. PMID: 40369555 Free PMC article.
-
Interstitial lung abnormalities and interstitial lung diseases associated with cigarette smoking in a rural cohort undergoing surgical resection.BMC Pulm Med. 2022 Apr 29;22(1):172. doi: 10.1186/s12890-022-01961-9. BMC Pulm Med. 2022. PMID: 35488260 Free PMC article.
-
Smoking duration alone provides stronger risk estimates of chronic obstructive pulmonary disease than pack-years.Thorax. 2018 May;73(5):414-421. doi: 10.1136/thoraxjnl-2017-210722. Epub 2018 Jan 11. Thorax. 2018. PMID: 29326298 Free PMC article.
-
Smoking-related idiopathic interstitial pneumonia: A review.Respirology. 2016 Jan;21(1):57-64. doi: 10.1111/resp.12576. Epub 2015 Jul 2. Respirology. 2016. PMID: 26138798 Review.
-
Respiratory bronchiolitis/interstitial lung disease: fibrosis, pulmonary function, and evolving concepts.Arch Pathol Lab Med. 2010 Jan;134(1):27-32. doi: 10.5858/134.1.27. Arch Pathol Lab Med. 2010. PMID: 20073602 Review.
Cited by
-
Rate of incidental findings on routine preoperative computed tomography for shoulder arthroplasty.Clin Shoulder Elb. 2024 Jun;27(2):169-175. doi: 10.5397/cise.2023.00836. Epub 2024 Mar 22. Clin Shoulder Elb. 2024. PMID: 38556913 Free PMC article.
-
Impact of coal mine dust exposure and cigarette smoking on lung disease in Appalachian coalminers.Respir Res. 2025 May 14;26(1):184. doi: 10.1186/s12931-025-03260-3. Respir Res. 2025. PMID: 40369555 Free PMC article.
-
Differences and Risk Factors of Peripheral Blood Immune Cells in Patients with Obstructive Sleep Apnea.Nat Sci Sleep. 2024 Jun 10;16:737-749. doi: 10.2147/NSS.S458098. eCollection 2024. Nat Sci Sleep. 2024. PMID: 38882924 Free PMC article.
-
Combined Predictors for the Diagnostic Transition from Acute and Transient Psychotic Disorder to Schizophrenia: A Retrospective Study.Neuropsychiatr Dis Treat. 2024 Oct 27;20:2029-2037. doi: 10.2147/NDT.S470127. eCollection 2024. Neuropsychiatr Dis Treat. 2024. PMID: 39484077 Free PMC article.
-
Mechanisms of Astragalus membranaceus (Fisch.) Bge. var. mongholicus (Bge.) Hsiao (huang qi) and Angelica sinensis (Oliv.) Diels (dang gui) in Ameliorating Hypoxia and Angiogenesis to Delay Pulmonary Nodule Malignant Transformation.Integr Cancer Ther. 2025 Jan-Dec;24:15347354241311917. doi: 10.1177/15347354241311917. Integr Cancer Ther. 2025. PMID: 39882753 Free PMC article. Review.
References
-
- CDC. Health effects of cigarette smoking; 2022. Available from: https://www.cdc.gov/tobacco/data_statistics/fact_sheets/health_effects/e.... Accessed August 24, 2022.
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
