

Anatomic Acromioclavicular Joint Reconstruction with and without Acromioclavicular Ligament Reconstruction: A Comparative Biomechanical Study
- PMID: 37035618
- PMCID: PMC10078810
- DOI: 10.1177/17585732211068322
Anatomic Acromioclavicular Joint Reconstruction with and without Acromioclavicular Ligament Reconstruction: A Comparative Biomechanical Study
Abstract
Background: The purpose of this study was to determine if adding a reconstructed superior acromioclavicular (AC) joint ligament adds significant biomechanical stability to the AC joint over anatomic coracoclavicular (CC) ligament reconstruction alone.
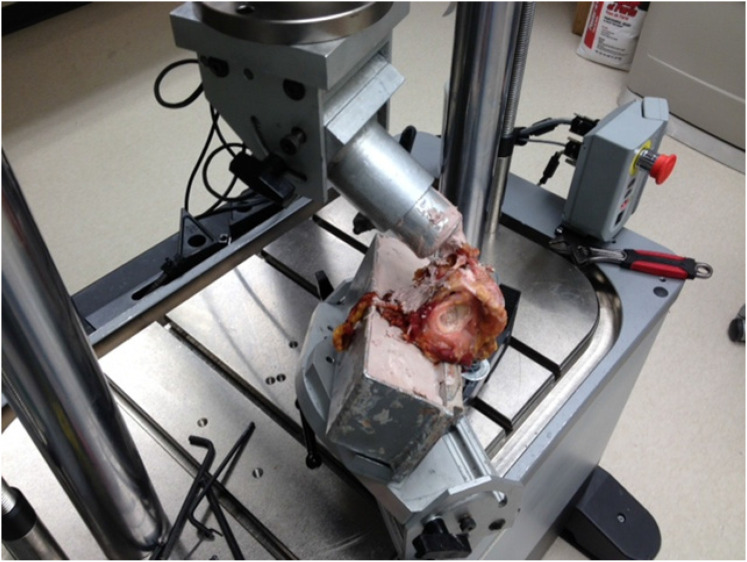
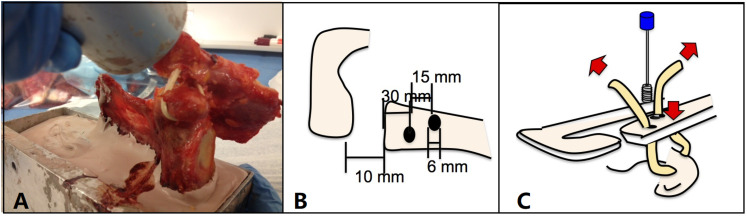
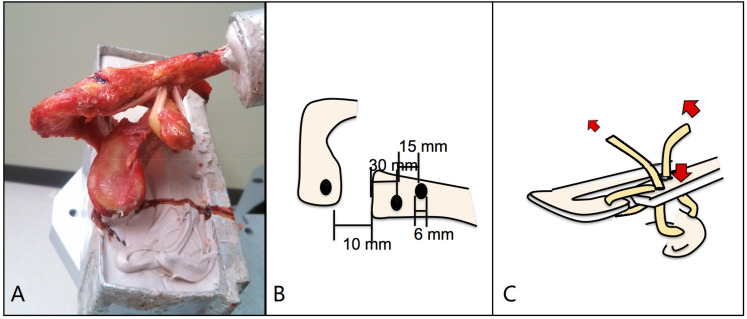
Methods: Fourteen cadaver shoulders were used for the comparison of biomechanical stability among the anatomic CC ligament reconstruction alone, CC and AC ligament reconstruction, and the intact groups by measuring the displacement under cyclic loads. A load to failure test was then performed in the vertical direction at a loading rate of 2 mm /sec to determine surgical-repair joints' tolerance to the maximum failure load.
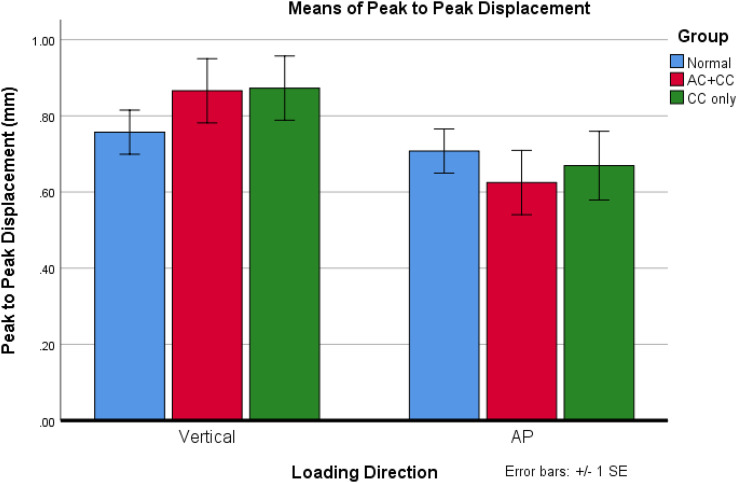
Results: The average peak-to-peak displacement induced by cyclic load in the sagittal axis and vertical axis direction was not significantly different between CC ligament reconstruction, CC and AC ligament reconstruction, and intact groups. The maximum failure load for the CC reconstruction (224.9 ± 91.8 N (Mean ± SEM)) was lower than CC/AC reconstruction groups (326.2 ± 123.3 N). The CC/AC reconstruction group failed at a significantly higher load (t test, p = 0.016) than the CC reconstruction group.
Conclusion: CC/AC reconstruction surgical technique yielded a better shoulder stability than CC ligament alone reconstruction that may better maintain reduction of the AC joint.Level of Evidence: Level II.
Keywords: acromioclavicular joint; biomechanics; coracoclavicular ligament; injury; reconstruction.
© The Author(s) 2022.
Conflict of interest statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
References
-
- Rockwood CJ, Williams G, Young D. Disorders of the acromioclavicular join. In: Rockwood CJ, Matsen FA, eds. The Shoulder. Philadelphia: WB Saunders, 1998: 483–553.
-
- Murena L, Canton G, Vulcano E, et al.Scapular dyskinesis and SICK scapula syndrome following surgical treatment of type III acute acromioclavicular dislocations. Knee Surg Sports Traumatol Arthrosc 2013; 21: 1146–1150. - PubMed
-
- Trainer G, Arciero RA, Mazzocca AD. Practical management of grade III acromioclavicular separations. Clin J Sport Med 2008; 18: 162–166. - PubMed
-
- Weaver JK, Dunn HK. Treatment of acromioclavicular injuries, especially complete acromioclavicular separation. J Bone Joint Surg Am 1972; 54: 1187–1194. - PubMed
LinkOut - more resources
Full Text Sources