

The perioperative outcomes of uniportal robotic-assisted thoracic surgeries-a systematic review and meta-analysis of surgical cohort studies and case reports
- PMID: 37035647
- PMCID: PMC10080331
- DOI: 10.21037/acs-2023-urats-37
The perioperative outcomes of uniportal robotic-assisted thoracic surgeries-a systematic review and meta-analysis of surgical cohort studies and case reports
Abstract
Background: Early results have illustrated the multiportal robotic approach to be safe and oncologically efficacious in the treatment of thoracic malignancies. Industry leaders have improved upon the lessons learned during the early multiportal studies and have now come to establish the feasibility of the biportal, and subsequently the uniportal robotic-assisted approach, all in an effort to offer patients equivalent or better outcomes with less surgical trauma. No current, coherent body of evidence currently exists outlining the early-term outcomes of patients undergoing uniportal robotic-assisted thoracic surgery. This systematic review and meta-analysis sought to clarify the early-phase outcomes of these patients.
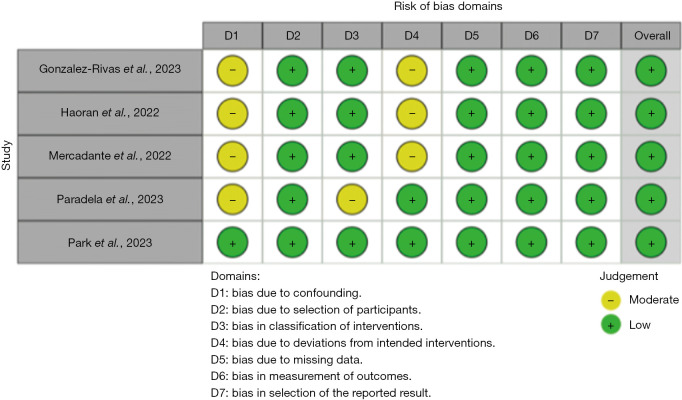
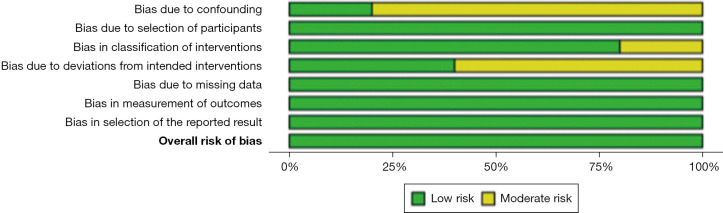
Methods: An electronic search of four databases was performed to identify relevant studies outlining the immediate post-operative outcomes of patients undergoing uniportal robotic-assisted thoracic surgeries. The primary endpoint was defined as technical success (i.e., no conversion to secondary robotic, video-assisted thoracoscopic, or open approaches). Secondary endpoints of interest included post-operative outcomes and complication rates. A meta-analysis using a random effects model of proportions or means was applied, as appropriate.
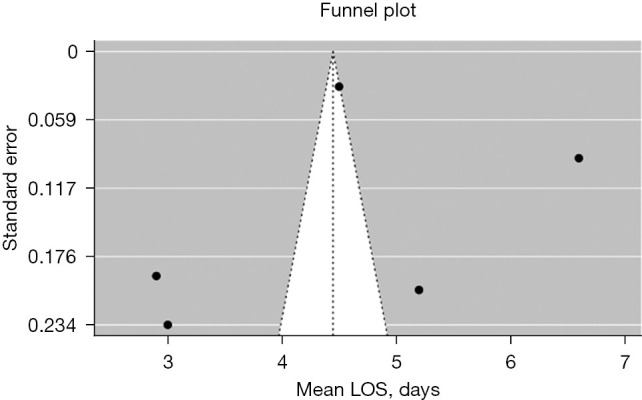
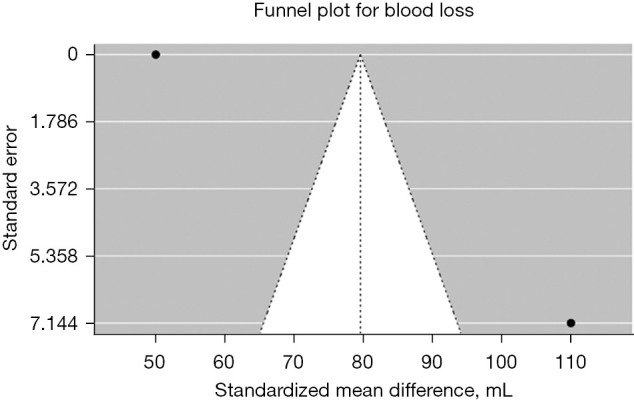
Results: The search strategy ultimately yielded 12 relevant studies for inclusion. A total of 240 patients (52% male) split across cohort studies and case reports were identified. The mean age of the two groups was 59.7±3.0 and 58.1±6.8 years, respectively. The mean operative time was 133.8±38.2 and 150.0±52.2 minutes, respectively. Length of hospital stay was 4.4±1.6 and 4.3±1.1 days, respectively. The mean blood loss was 80.0±25.1 mL The majority of identified procedures were lobectomies, segmentectomies, and wedge resections, though complex sleeve resections and anterior mediastinal mass resections were also completed. Cumulative technical success was 99.9%.
Conclusions: The uniportal robotic-assisted approach, when completed in expert hands, has been illustrated to have exceedingly low rates of conversion to secondary procedures, along with short length of stay (LOS), minimal blood loss, and short procedural times (variable depending on operation type). Current evidence on the feasibility of this approach will be bolstered by upcoming multi-institutional series.
Keywords: Robotic thoracic surgery; early outcomes; lobectomy; wedge resection.
2023 Annals of Cardiothoracic Surgery. All rights reserved.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures

Similar articles
-
The learning curve of the robotic-assisted lobectomy-a systematic review and meta-analysis.Ann Cardiothorac Surg. 2023 Jan 31;12(1):1-8. doi: 10.21037/acs-2022-urats-14. Epub 2023 Jan 14. Ann Cardiothorac Surg. 2023. PMID: 36793987 Free PMC article.
-
Comparison of uniportal robotic-assisted thoracic surgery pulmonary anatomic resections with multiport robotic-assisted thoracic surgery: a multicenter study of the European experience.Ann Cardiothorac Surg. 2023 Mar 31;12(2):102-109. doi: 10.21037/acs-2022-urats-27. Epub 2023 Mar 9. Ann Cardiothorac Surg. 2023. PMID: 37035654 Free PMC article.
-
Hybrid uniportal robotic-assisted thoracoscopic surgery using video-assisted thoracoscopic surgery staplers: technical aspects and results.Ann Cardiothorac Surg. 2023 Jan 31;12(1):34-40. doi: 10.21037/acs-2022-urats-140. Epub 2022 Dec 30. Ann Cardiothorac Surg. 2023. PMID: 36793988 Free PMC article.
-
Systematic review and meta-analysis of uniportal versus multiportal video-assisted thoracoscopic lobectomy for lung cancer.Ann Cardiothorac Surg. 2016 Mar;5(2):76-84. doi: 10.21037/acs.2016.03.17. Ann Cardiothorac Surg. 2016. PMID: 27134832 Free PMC article. Review.
-
Robotic-Assisted Videothoracoscopic Surgery of the Lung.Cancer Control. 2015 Jul;22(3):314-25. doi: 10.1177/107327481502200309. Cancer Control. 2015. PMID: 26351887 Review.
Cited by
-
Comparison of short-term outcomes between multi-arm uniportal and multiport robotic-assisted thoracoscopic surgery based on propensity score matching.World J Surg Oncol. 2025 Jun 9;23(1):224. doi: 10.1186/s12957-025-03881-4. World J Surg Oncol. 2025. PMID: 40490772 Free PMC article.
References
-
- Institute of Health Economics. Quality Appraisal of Case Series Study Tool. Institute of Health Economics, Edmonton; 2016.
LinkOut - more resources
Full Text Sources