

Imaging in patients with acute dyspnea when cardiac or pulmonary origin is suspected
- PMID: 37035768
- PMCID: PMC10077421
- DOI: 10.1259/bjro.20220026
Imaging in patients with acute dyspnea when cardiac or pulmonary origin is suspected
Abstract
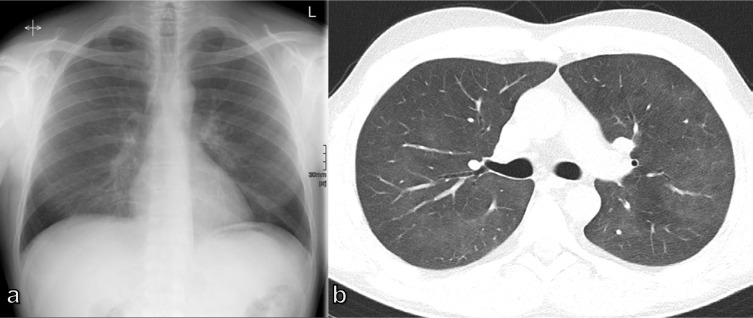
A wide spectrum of conditions, from life-threatening to non-urgent, can manifest with acute dyspnea, thus presenting major challenges for the treating physician when establishing the diagnosis and severity of the underlying disease. Imaging plays a decisive role in the assessment of acute dyspnea of cardiac and/or pulmonary origin. This article presents an overview of the current imaging modalities used to narrow the differential diagnosis in the assessment of acute dyspnea of cardiac or pulmonary origin. The current indications, findings, accuracy, and limits of each imaging modality are reported. Chest radiography is usually the primary imaging modality applied. There is a low radiation dose associated with this method, and it can assess the presence of fluid in the lung or pleura, consolidations, hyperinflation, pneumothorax, as well as heart enlargement. However, its low sensitivity limits the ability of the chest radiograph to accurately identify the causes of acute dyspnea. CT provides more detailed imaging of the cardiorespiratory system, and therefore, better sensitivity and specificity results, but it is accompanied by higher radiation exposure. Ultrasonography has the advantage of using no radiation, and is fast and feasible as a bedside test and appropriate for the assessment of unstable patients. However, patient-specific factors, such as body habitus, may limit its image quality and interpretability. Advances in knowledge This review provides guidance to the appropriate choice of imaging modalities in the diagnosis of patients with dyspnea of cardiac or pulmonary origin.
© 2023 The Authors. Published by the British Institute of Radiology.
Conflict of interest statement
Competing interests: Ruxandra-Iulia Milos, Carmen Bartha, Benedikt H. Heidinger, Florian Prayer, Lucian Beer, Christian Wassipaul, Daria Kifjak, Martin Watzenböck – no conflict of interests to declare; Sebastian Röhrich – consulting activities contextflow GmbH; Helmut Prosch – Speaker honoria: AstraZeneca, BMS, Boehringer Ingelheim, Siemens Healthcare, Takeda. Research grants: Boehringer Ingelheim
Figures










References
-
- Cairns C, Kang K, L S. National Hospital Ambulatory Medical Care Survey: 2018 emergency department summary tables. Available from: https://www.cdc.gov/nchs/data/nhamcs/web_tables/2018_ed_web_tables-508.pdf
Publication types
LinkOut - more resources
Full Text Sources
