

Multi-modality parathyroid imaging: A shifting paradigm
- PMID: 37035829
- PMCID: PMC10080580
- DOI: 10.4329/wjr.v15.i3.69
Multi-modality parathyroid imaging: A shifting paradigm
Abstract
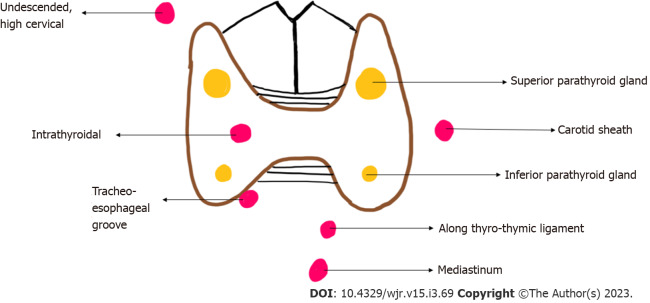
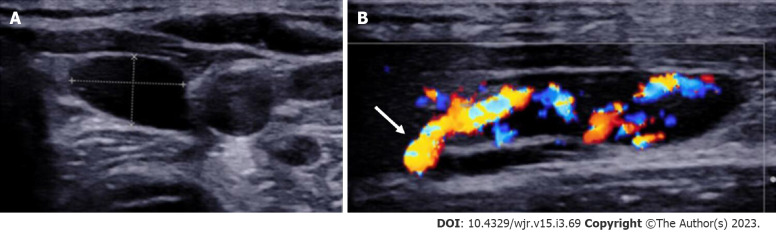
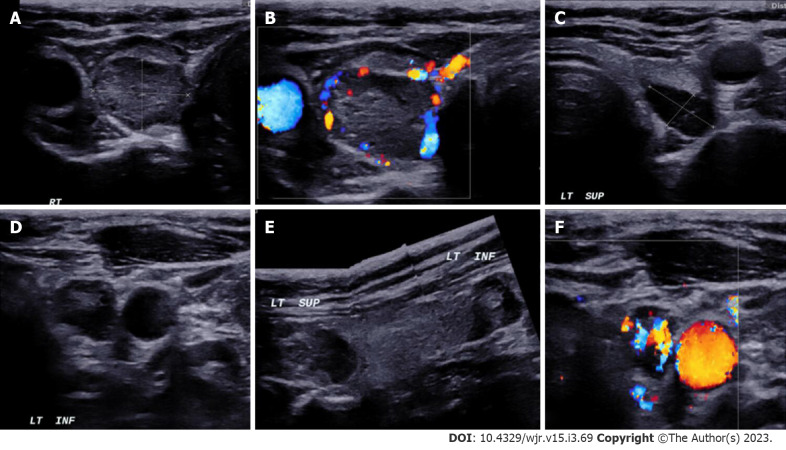
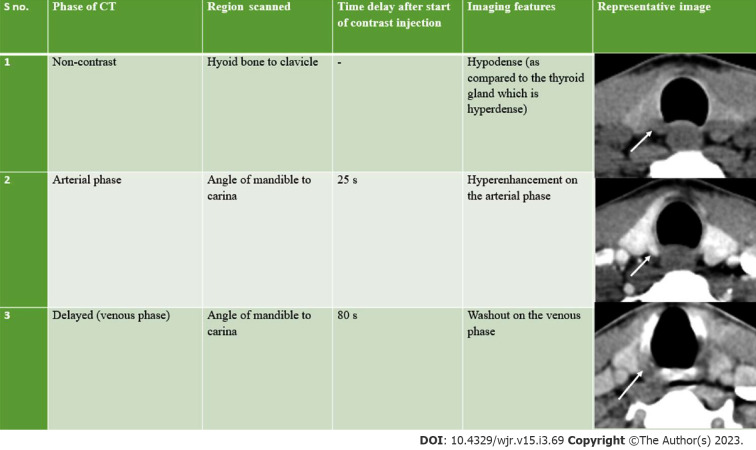
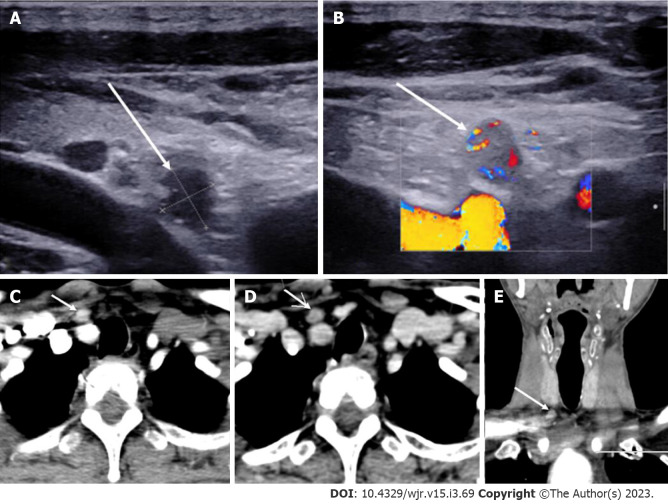
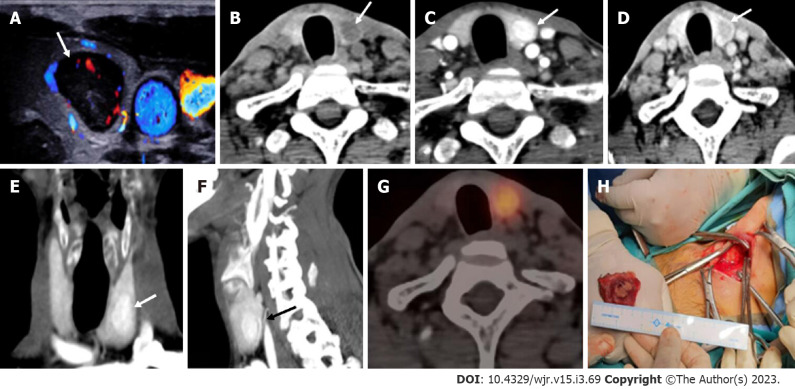
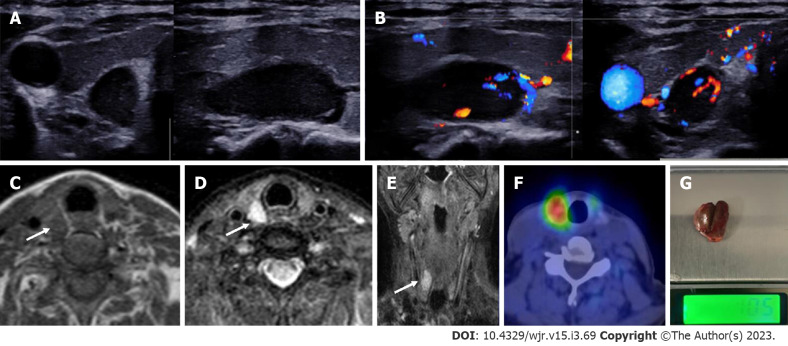
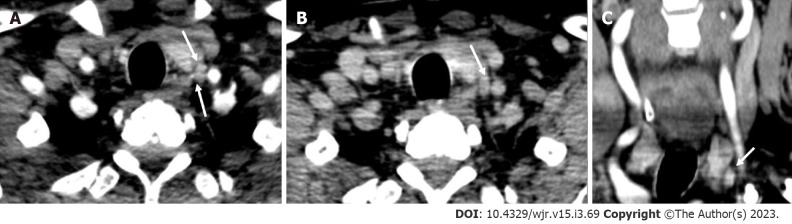
The goal of parathyroid imaging in hyperparathyroidism is not diagnosis, rather it is the localization of the cause of hyperparathyroidism for planning the best therapeutic approach. Hence, the role of imaging to accurately and precisely localize the abnormal parathyroid tissue is more important than ever to facilitate minimally invasive parathyroidectomy over bilateral neck exploration. The common causes include solitary parathyroid adenoma, multiple parathyroid adenomas, parathyroid hyperplasia and parathyroid carcinoma. It is highly imperative for the radiologist to be cautious of the mimics of parathyroid lesions like thyroid nodules and lymph nodes and be able to differentiate them on imaging. The various imaging modalities available include high resolution ultrasound of the neck, nuclear imaging studies, four-dimensional computed tomography (4D CT) and magnetic resonance imaging. Contrast enhanced ultrasound is a novel technique which has been recently added to the armamentarium to differentiate between parathyroid adenomas and its mimics. Through this review article we wish to review the imaging features of parathyroid lesions on various imaging modalities and present an algorithm to guide their radiological differentiation from mimics.
Keywords: Contrast enhanced ultrasound; Four-dimensional computed tomography; Magnetic resonance imaging; Nuclear Imaging; Parathyroid adenoma; Ultrasound.
©The Author(s) 2023. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: All the authors declare that they have no conflict of interest.
Figures

References
-
- Fraser WD. Hyperparathyroidism. Lancet. 2009;374:145–158. - PubMed
-
- Bunch PM, Kelly HR. Preoperative Imaging Techniques in Primary Hyperparathyroidism: A Review. JAMA Otolaryngol Head Neck Surg. 2018;144:929–937. - PubMed
-
- Bilezikian JP, Bandeira L, Khan A, Cusano NE. Hyperparathyroidism. Lancet. 2018;391:168–178. - PubMed
-
- Bunch PM, Randolph GW, Brooks JA, George V, Cannon J, Kelly HR. Parathyroid 4D CT: What the Surgeon Wants to Know. Radiographics. 2020;40:1383–1394. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
