

Iatrogenic Cerebral Amyloid Angiopathy Post Neurosurgery: Frequency, Clinical Profile, Radiological Features, and Outcome
- PMID: 37035916
- PMCID: PMC10121246
- DOI: 10.1161/STROKEAHA.122.041690
Iatrogenic Cerebral Amyloid Angiopathy Post Neurosurgery: Frequency, Clinical Profile, Radiological Features, and Outcome
Abstract
Background: Prion-like transmission of amyloid-ß through cadaveric dura, decades after neurosurgical procedures, has been hypothesized as an iatrogenic cause of cerebral amyloid angiopathy (CAA). We investigated new and previously described patients to assess the clinical profile, radiological features, and outcome of this presumed iatrogenic CAA-subtype (iCAA).
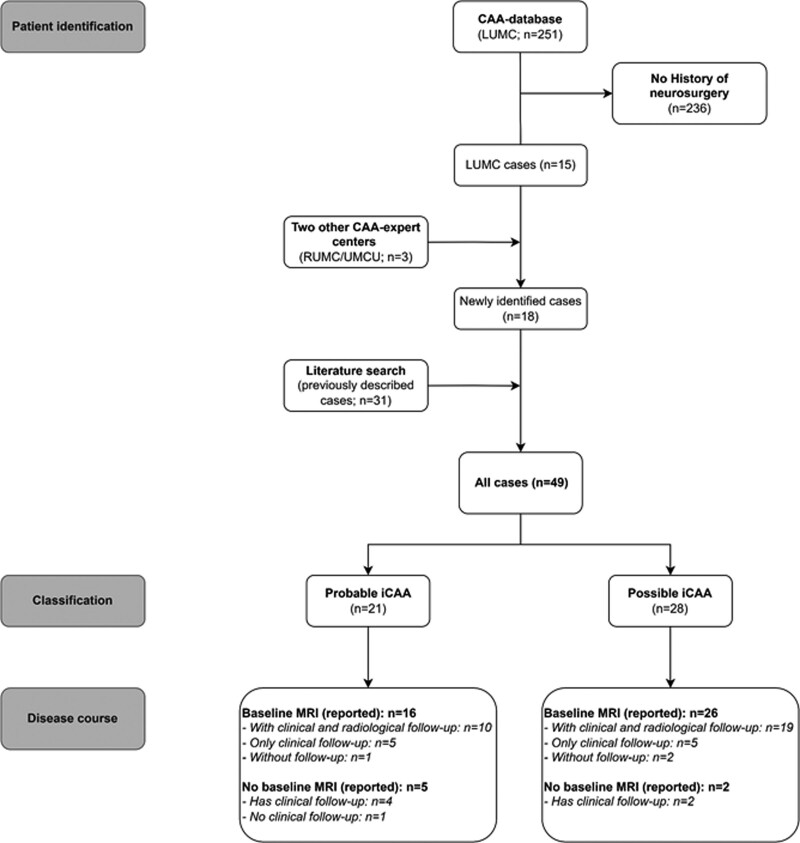
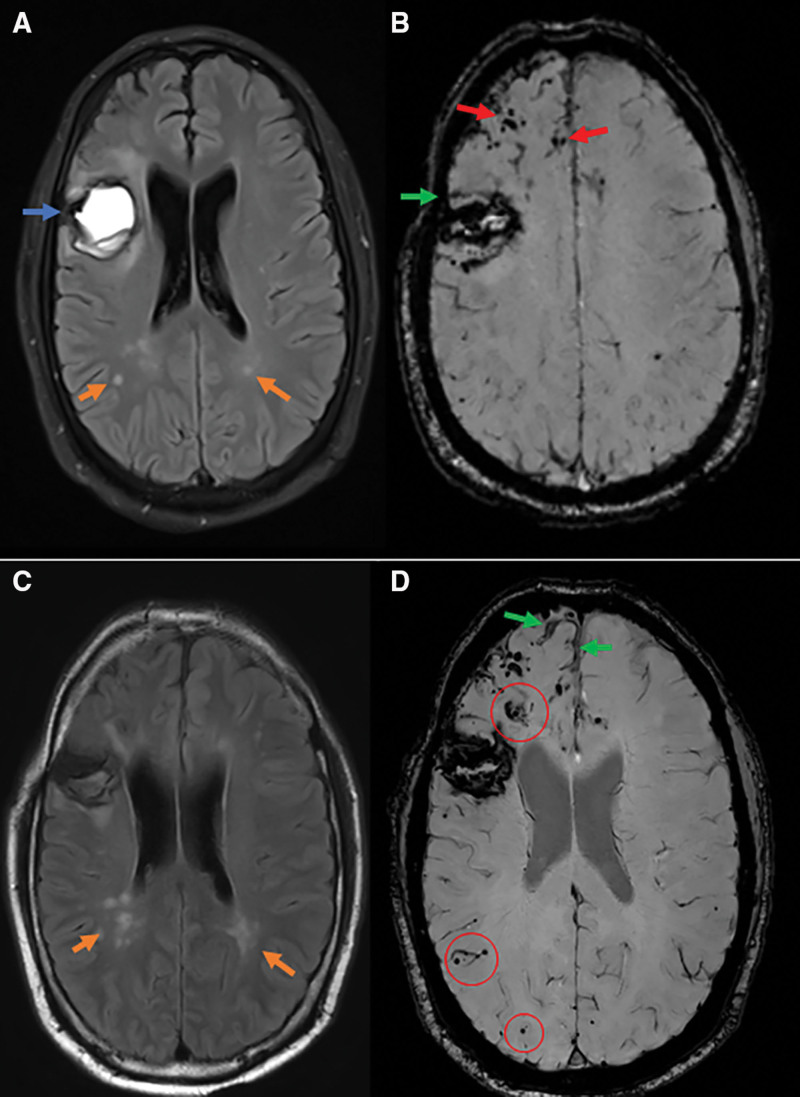
Methods: Patients were collected from our prospective lobar hemorrhage and CAA database (n=251) with patients presenting to our hospital between 2008 and 2022. In addition, we identified patients with iCAA from 2 other Dutch CAA-expertise hospitals and performed a systematic literature-search for previously described patients. We classified patients according to the previously proposed diagnostic criteria for iCAA, assessed clinical and radiological disease features, and calculated intracerebral hemorrhage (ICH)-recurrence rates. We evaluated the spatial colocalization of cadaveric dura placement and CAA-associated magnetic resonance imaging markers.
Results: We included 49 patients (74% men, mean age 43 years [range, 27-84]); 15 from our database (6% [95% CI, 3%-10%]; 45% of patients <55 years), 3 from the 2 other CAA-expertise hospitals, and 31 from the literature. We classified 43% (n=21; 1 newly identified patient) as probable and 57% (n=28) as possible iCAA. Patients presented with lobar ICH (57%), transient focal neurological episodes (12%), or seizures (8%). ICH-recurrence rate in the new patients (16/100 person-years [95% CI, 7-32], median follow-up 18 months) was lower than in the previously described patients (77/100 person-years [95% CI, 59-99], median follow-up 18 months). One patient had a 10 year interlude without ICH-recurrence. We identified no clear spatial relationship between dura placement and CAA-associated magnetic resonance imaging markers. During follow-up (median, 18 months), 20% of the patients developed transient focal neurological episodes and 20% cognitively declined.
Conclusions: iCAA seems common in patients presenting with nonhereditary CAA under the age of 55. Clinical and radiological features are comparable with sCAA. After diagnosis, multiple ICH-recurrences but also long symptom-free intervals can occur. Harmonized registries are necessary to identify and understand this potentially underrecognized CAA-subtype.
Keywords: amyloid; cerebral amyloid angiopathy; cerebral hemorrhage; human growth hormone; magnetic resonance imaging; neurosurgery; prions.
Conflict of interest statement
Dr Wermer reports independent support from the Netherlands Organization for Scientific Research (NWO VIDI grant 9171337), the Dutch Research Council (NWO memorable BIONIC [Biomarkers for Cognitive Impairment due to Cerebral Amyloid Angiopathy] 733050822), the Dutch Heart Foundation (Clinical Established Investigator grant 2016T86), the Dutch Brain Foundation and the Dutch cerebral amyloid angiopathy (CAA) foundation. Dr Terwindt reports independent support from the Dutch Research Council (Nederlandse Organisatie voor Wetenschappelijk Onderzoek memorable BIONIC 733050822), the Dutch Heart Foundation, the Dutch Brain Foundation and the Dutch CAA foundation. Dr Schreuder reports independent support from the Dutch Heart Foundation (Senior Clinical Scientist grant 2019T060), the Dutch Heart Foundation and the Swedisch Orphan Biovitrum AB. Dr Klijn reports disclosures all unrelated to this study: support from the Netherlands Cardiovascular Research Initiative, which is supported by the Dutch Heart Foundation, CVON2015-01: CONTRAST (Collaboration for New Treatments of Acute Stroke), and the support of the Brain Foundation Netherlands (HA2015.01.06). The collaboration project is additionally financed by the Ministry of Economic Affairs by means of the public-private partnerships allowance made available by the Top Sector Life Sciences & Health to stimulate public-private partnerships (LSHM17016). This work was funded in part through unrestricted funding by Stryker, Medtronic, and Cerenovus; the funding sources were not involved in study design, monitoring, data collection, statistical analyses, interpretation of results, or article writing. Radboud University Medical Center and Erasmus MC received additional unrestricted funding on behalf of CONTRAST, for the execution of the Dutch Intracerebral Hemorrhage (ICH) Surgery Trial pilot study from Penumbra Inc. For the Dutch ICH Surgery Trial, they also received a grant from ZonMw/Promising care (grant 80- 86200-08-25001). The other authors report no conflicts.
Figures
Comment in
-
Seed to Bleed: Iatrogenic Cerebral Amyloid Angiopathy.Stroke. 2023 May;54(5):1224-1226. doi: 10.1161/STROKEAHA.123.042583. Epub 2023 Apr 10. Stroke. 2023. PMID: 37035915 Free PMC article. No abstract available.
References
-
- Hamaguchi T, Taniguchi Y, Sakai K, Kitamoto T, Takao M, Murayama S, Iwasaki Y, Yoshida M, Shimizu H, Kakita A, et al. . Significant association of cadaveric dura mater grafting with subpial Aβ deposition and meningeal amyloid angiopathy. Acta Neuropathol. 2016;132:313–315. doi: 10.1007/s00401-016-1588-3 - PubMed
-
- Hervé D, Porché M, Cabrejo L, Guidoux C, Tournier-Lasserve E, Nicolas G, Adle-Biassette H, Plu I, Chabriat H, Duyckaerts C. Fatal Aβ cerebral amyloid angiopathy 4 decades after a dural graft at the age of 2 years. Acta Neuropathol. 2018;135:801–803. doi: 10.1007/s00401-018-1828-9 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
