

Successful Early Neovascularization in Composite Tracheal Grafts
- PMID: 37036314
- PMCID: PMC10524236
- DOI: 10.1002/ohn.350
Successful Early Neovascularization in Composite Tracheal Grafts
Abstract
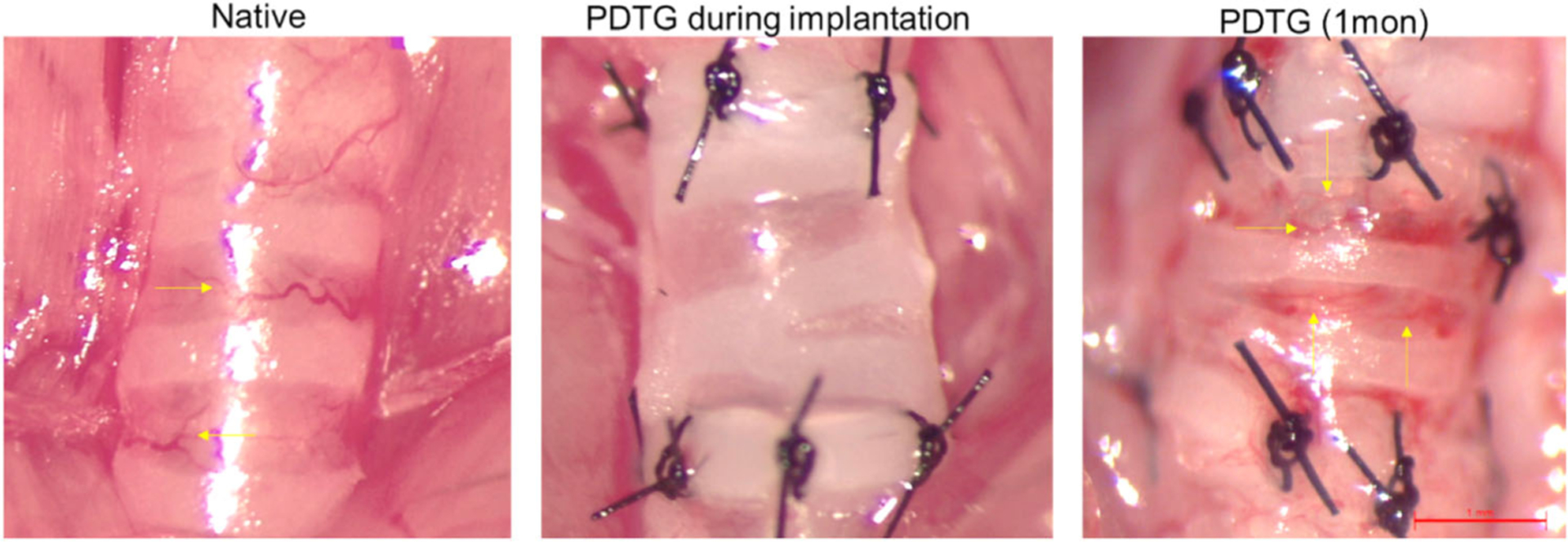
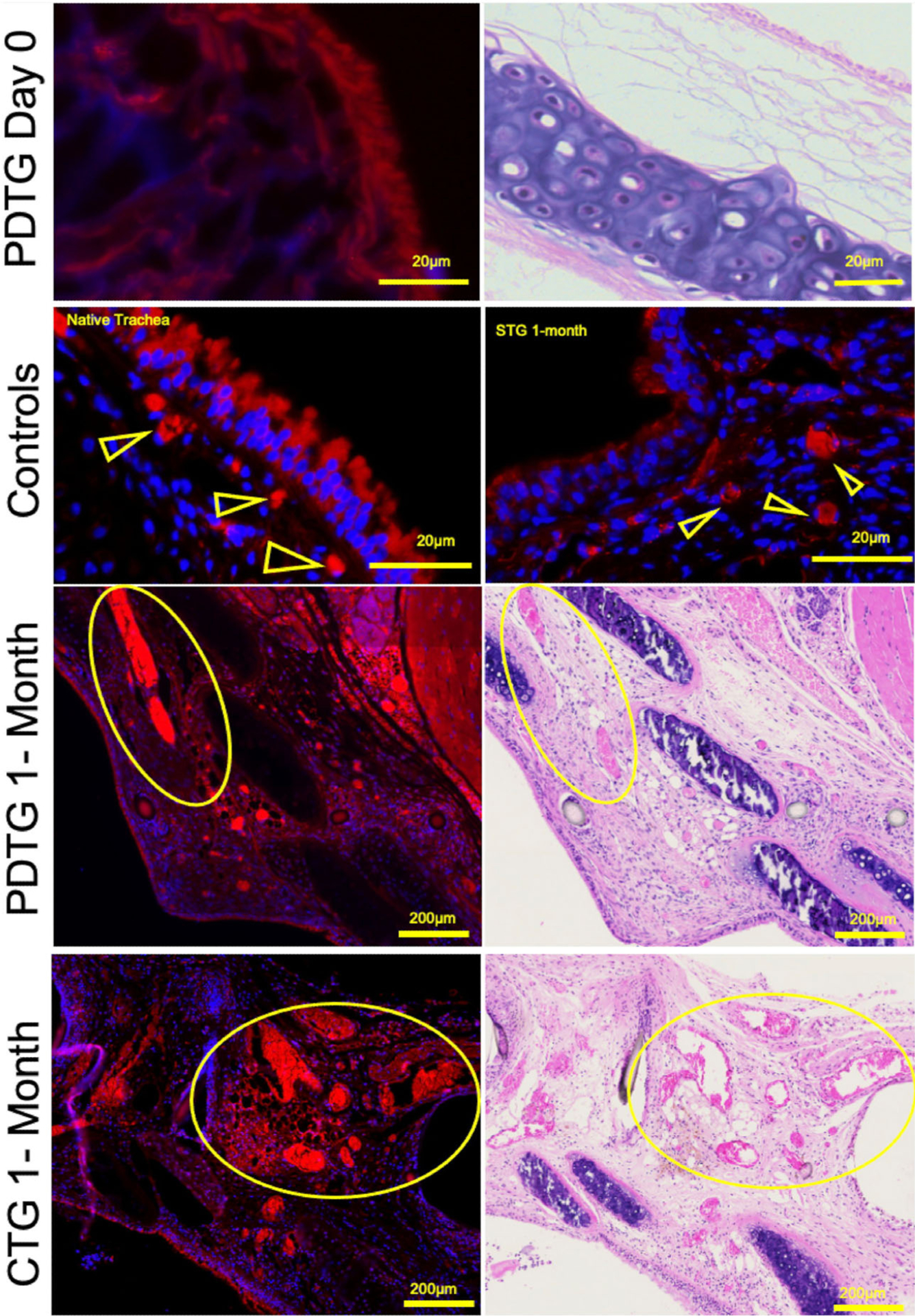
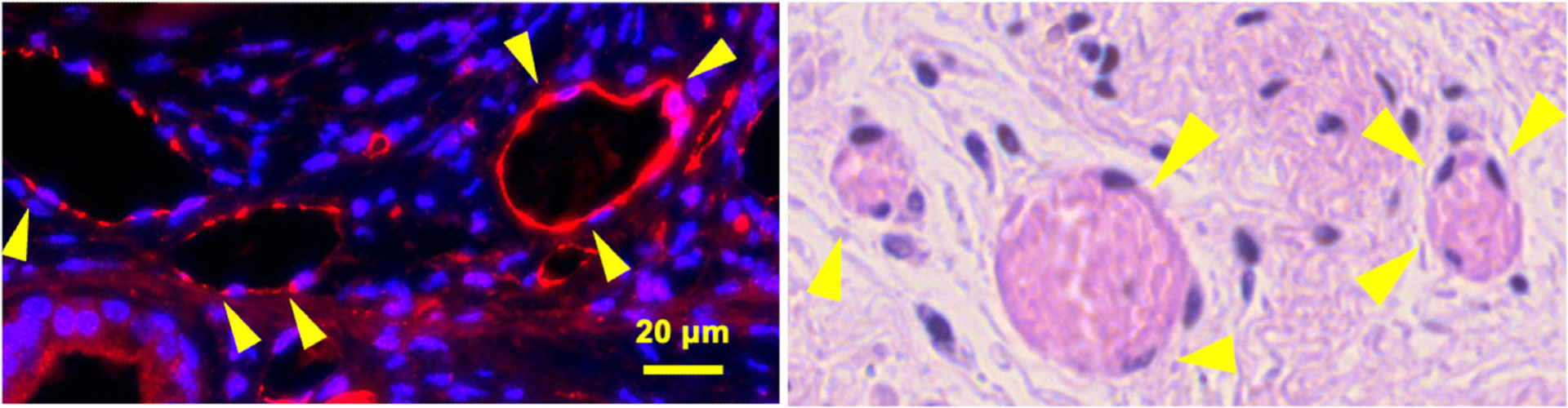
Objective: Long-segment tracheal defects require tissue replacement for successful reconstruction. Rapid revascularization is imperative to maintain graft function. We previously showed that partially decellularized tracheal grafts (PDTG) and composite tracheal grafts (CTG; PDTG supported by a 3-dimensionally printed external splint) regenerate respiratory epithelium and may support the regeneration of endothelial cells (CD31+). However, the capability of graft endothelial cells to organize or contribute to tracheal revascularization remains unclear. In this study, we quantified endothelial cells (CD31+) and neovessel formation in PDTG and CTG. We hypothesize that PDTG and CTG support tracheal neovascularization to a similar extent as surgical (syngeneic tracheal graft [STG]) and native trachea (NT) controls.
Study design: The animal study, a randomized control trial.
Setting: Center for Regenerative Medicine, Nationwide Children's Hospital.
Methods: PDTG was created via an established decellularization protocol. Segmental tracheal reconstruction was performed with STG, PDTG, or CTG using a mouse microsurgical model. NT was used as a nonsurgical control. At 1 month, mice were euthanized, grafts harvested, sectioned, and stained with CD31 and hematoxylin and eosin. Neovessel formation was quantified by the number of formed blood vessels in the lamina propria and vessel size (vessel/graft area, mm2 ).
Results: Decellularization eliminated all endothelial cells and there were no perfused vessels at implantation. At 1 month, PDTG and CTG supported neovessel formation with tubular vessels lined with endothelial cells. There was no difference in the number or size of vessels compared to controls.
Conclusion: PDTG and CTG support tracheal endothelial cell regeneration and neovessel formation. Future directions to assess the function, kinetics, and distribution of graft neovessels are needed.
Keywords: neovascularization; tissue engineering; tracheal replacement.
© 2023 The Authors. Otolaryngology-Head and Neck Surgery published by Wiley Periodicals LLC on behalf of American Academy of Otolaryngology-Head and Neck Surgery Foundation.
Conflict of interest statement
Kyle K. VanKoevering—unrestricted research funding from KLS Martin, partial owner of MakeMedical. All other authors: Nothing to disclose.
Figures

References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
