

The Deep Fascia of the Head and Neck Revisited: Relationship with the Facial Nerve and Implications for Rhytidectomy
- PMID: 37036327
- PMCID: PMC11104498
- DOI: 10.1097/PRS.0000000000010556
The Deep Fascia of the Head and Neck Revisited: Relationship with the Facial Nerve and Implications for Rhytidectomy
Abstract
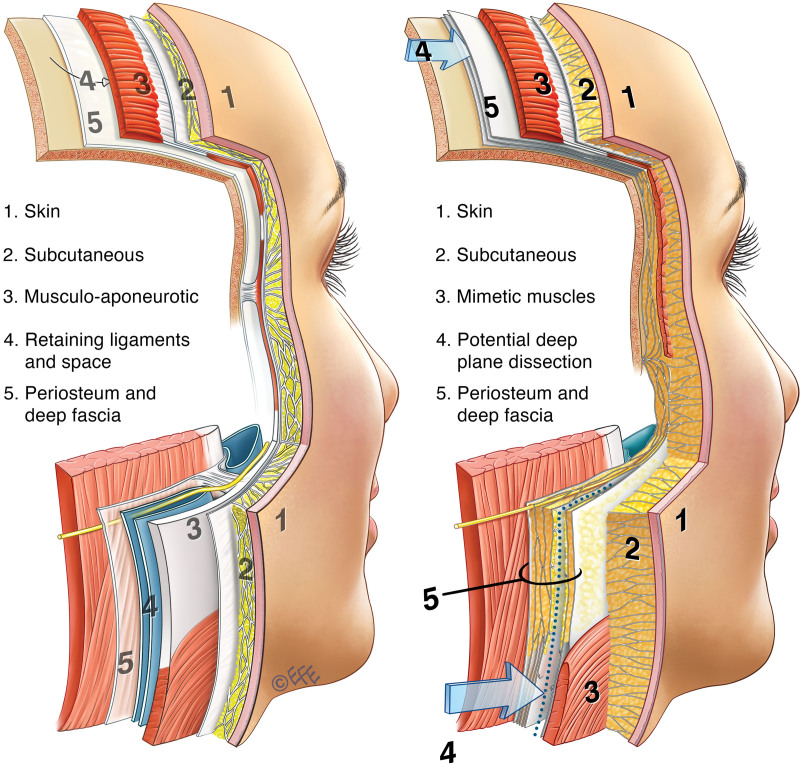
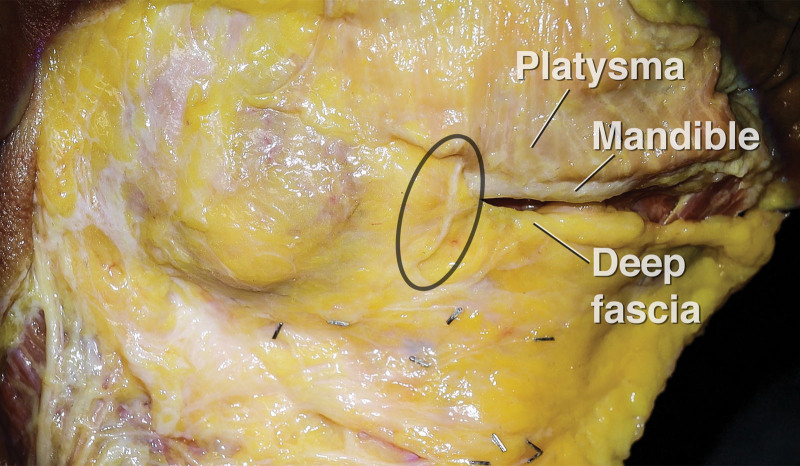
Background: The deep fascia is important in face-lift surgery, as it is relied on for protection of the facial nerve during surgical dissection. Lack of consistency with the term may be attributable to the term deep fascia having two different meanings. It is a specific type of connective tissue, classically thin, fibrous, and flat, whereas in the description of the layers of the face and neck, the deep fascia layer includes all the connective tissue deep to the superficial fascia layer. This cadaver study was undertaken to clarify the layered anatomy of the face and neck and its relationship with the facial nerve branches.
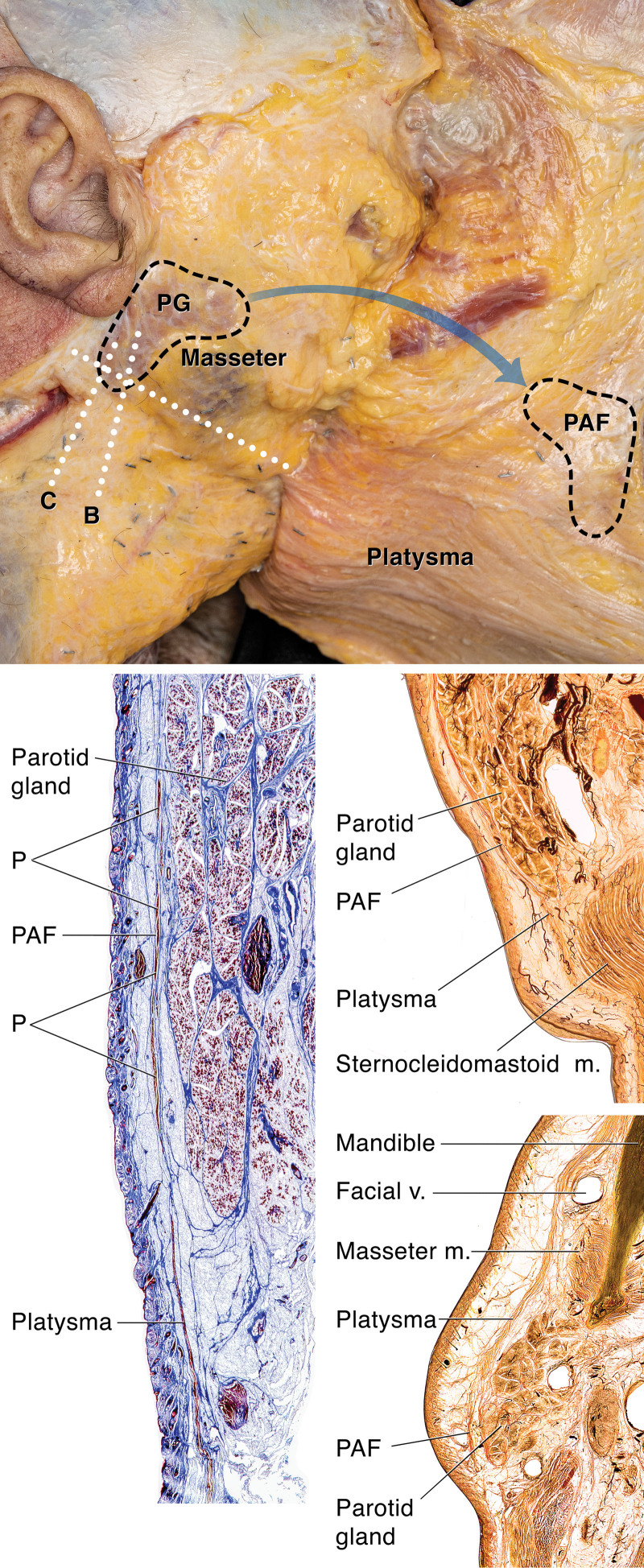
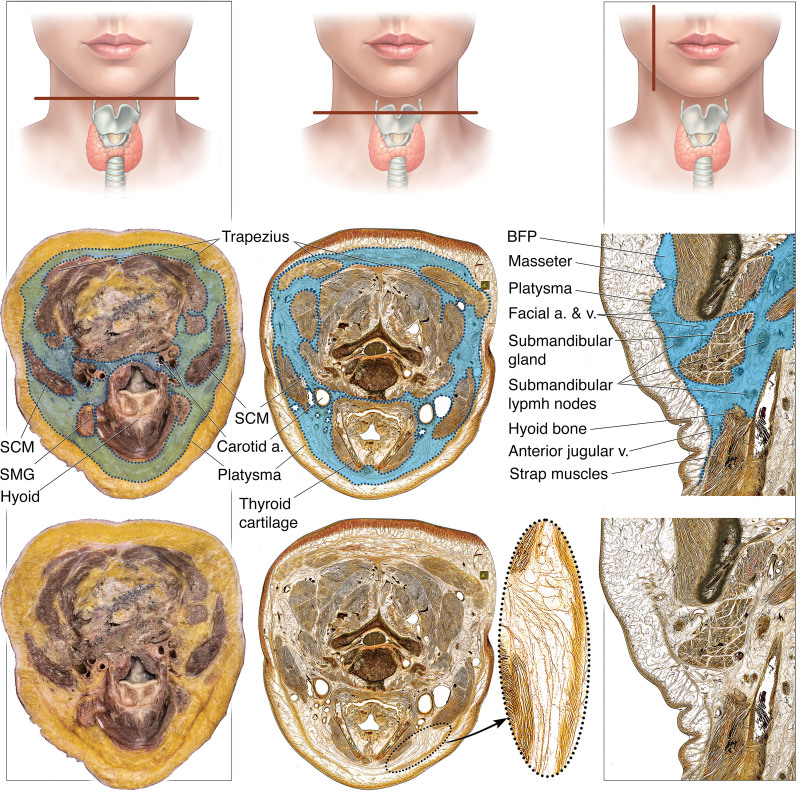
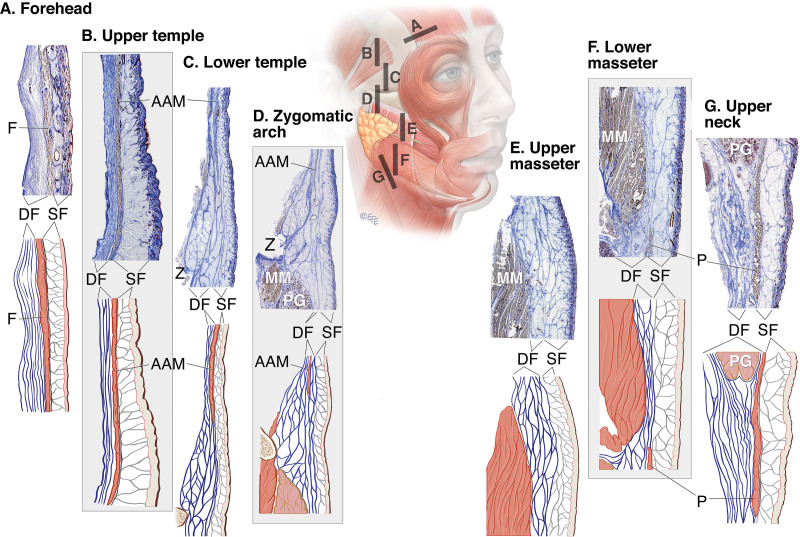
Methods: Preliminary dissections and macrosectioning, followed by a conclusive series of standardized layered dissections, histologic analysis, and sheet plastination, were performed on 50 cadaver heads.
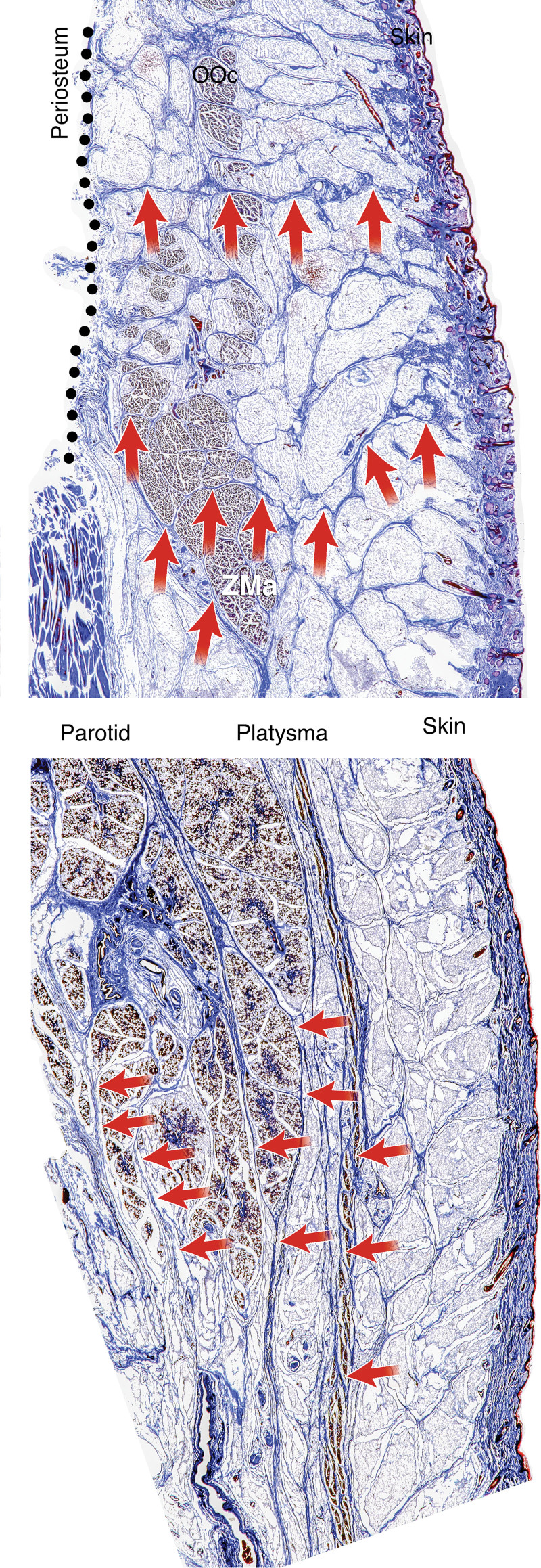
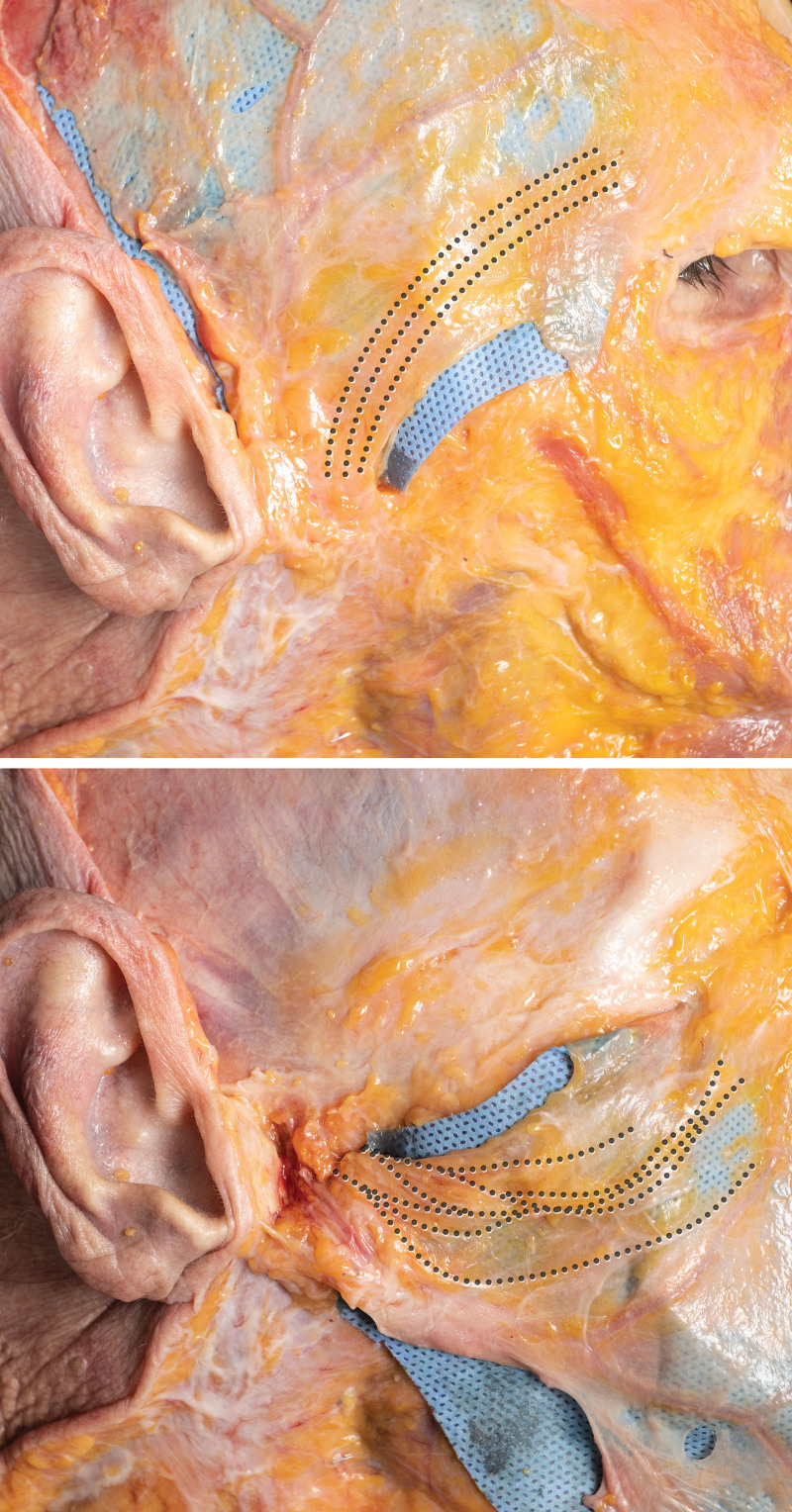
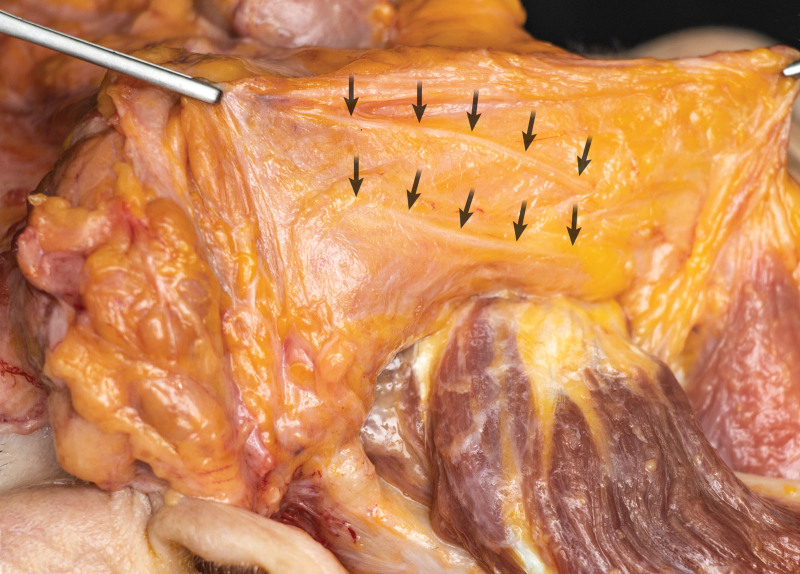
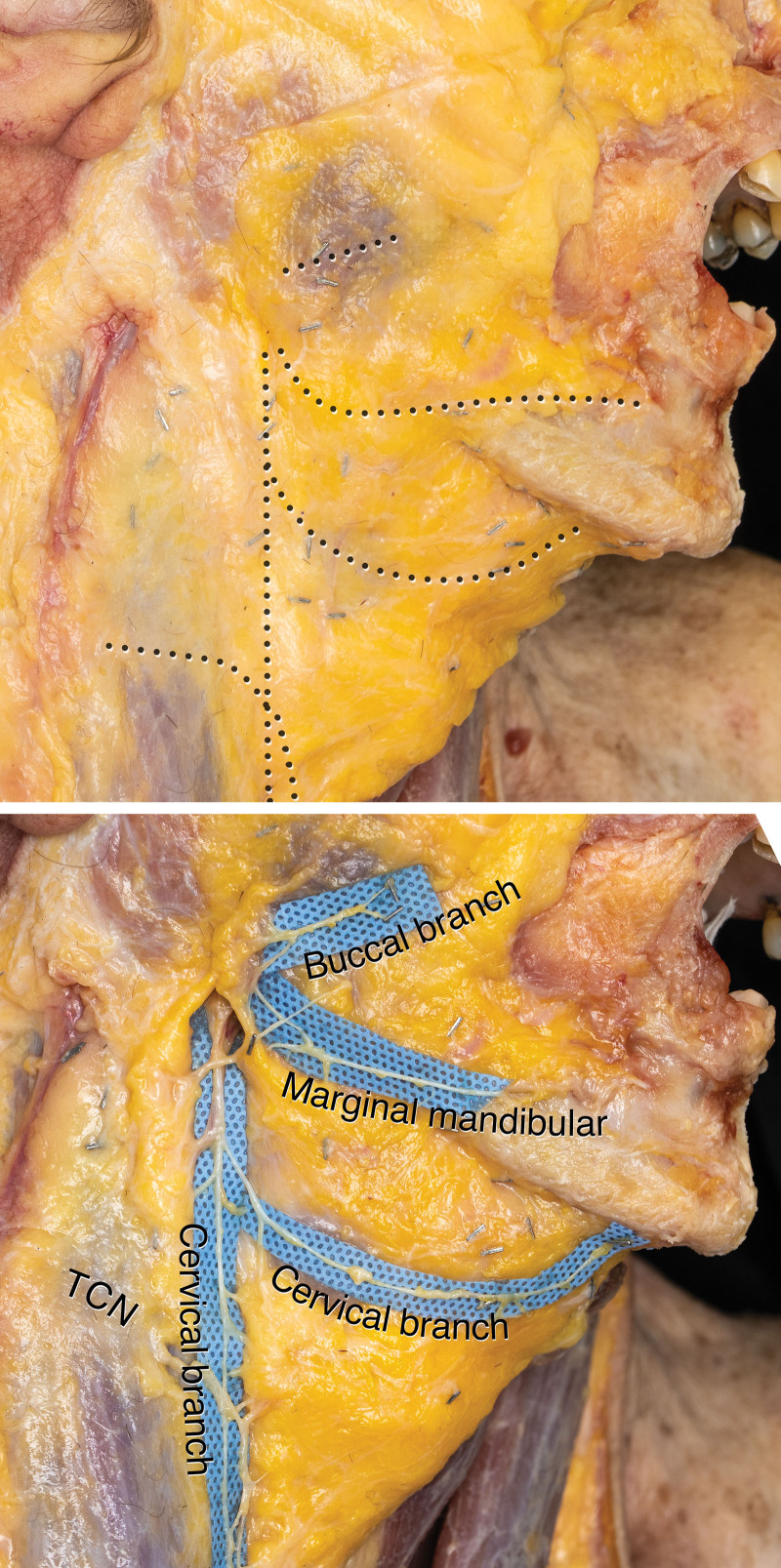
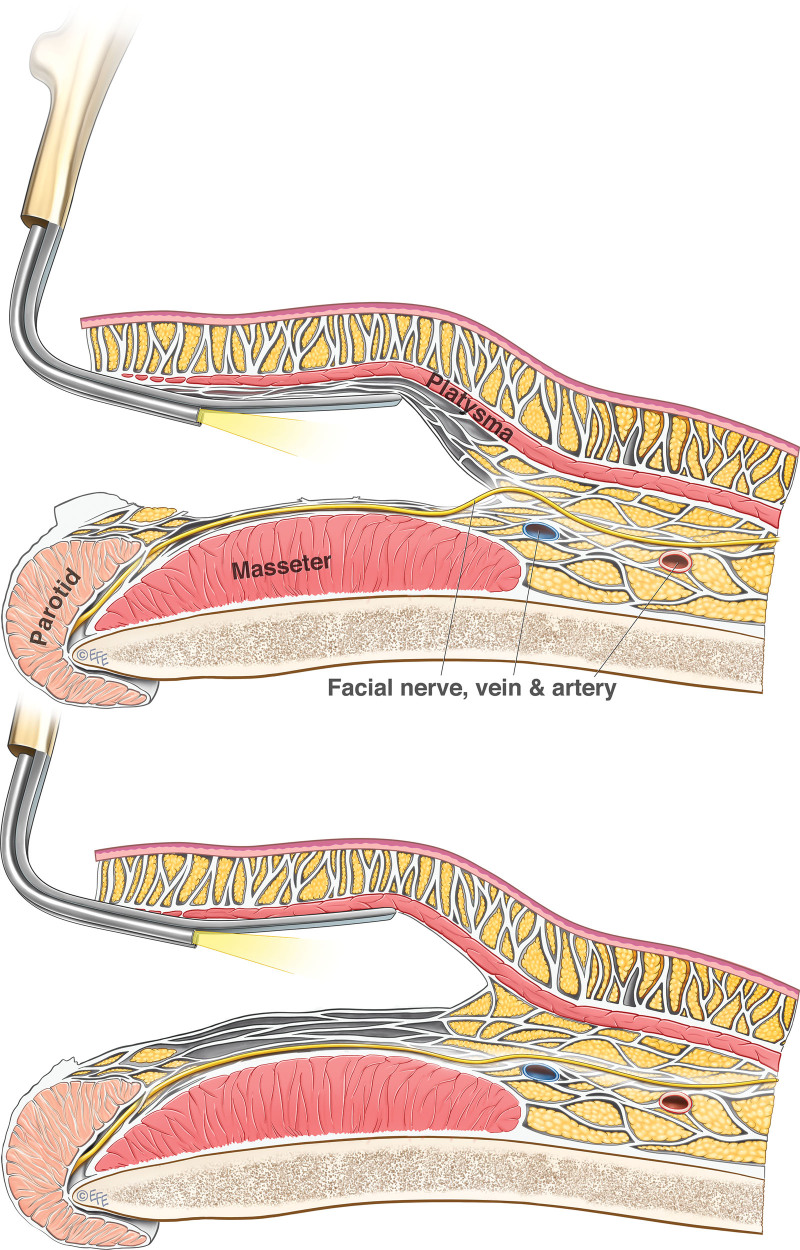
Results: The deep fascia is thin in convex areas of the face and neck, and thicker in concave areas; it is interspersed with deep fat. The facial nerve branches, after emerging from the parotid gland, are embedded within the deep fascia, not deep to it. They transition from deep within the deep fascia at specific locations to course in the most superficial part of the deep fascia where they underlie their target superficial fascia muscles and are at risk from deep plane face-lift dissection.
Conclusions: The deep fascia layer is a multilamellar fibrofatty layer of variable thickness, which includes the deep fat in which the facial nerve branches are embedded. In deep plane face-lift surgery, dissection must be performed in the most superficial level of this deep fascia layer.
Copyright © 2023 The Authors. Published by Wolters Kluwer Health, Inc. on behalf of the American Society of Plastic Surgeons.
Conflict of interest statement
The authors have no financial interests to disclose. No funding was received for this article.
Figures



References
-
- Burns A. Observations on the Surgical Anatomy of the Head and Neck. Edinburgh: Thomas Bryce & Co; 1811.
-
- Wendell-Smith CP. Fascia: an illustrative problem in international terminology. Surg Radiol Anat. 1997;19:273–277. - PubMed
-
- Mendelson BC, Wong CH. Anatomy of the aging face. In: Neligan PC, ed. Plastic Surgery. Philadelphia: Elsevier; 2013:78–92.
-
- Cotofana S, Fratila A, Schenck T, Redka-Swoboda W, Zilinsky I, Pavicic T. The anatomy of the aging face: a review. Facial Plast Surg. 2016;32:253–260. - PubMed
-
- Last RJ, McMinn RMH. Last’s Anatomy: Regional and Applied. McMinn RMH, ed. New York: Churchill Livingstone; 1992.
MeSH terms
LinkOut - more resources
Full Text Sources
