

Racial and Ethnic Disparities in Health Care Use and Access Associated With Loss of Medicaid Supplemental Insurance Eligibility Above the Federal Poverty Level
- PMID: 37036727
- PMCID: PMC10087092
- DOI: 10.1001/jamainternmed.2023.0512
Racial and Ethnic Disparities in Health Care Use and Access Associated With Loss of Medicaid Supplemental Insurance Eligibility Above the Federal Poverty Level
Abstract
Importance: Medicaid supplemental insurance covers most cost sharing in Medicare. Among low-income Medicare beneficiaries, the loss of Medicaid eligibility above this program's income eligibility threshold (100% of federal poverty level [FPL]) may exacerbate racial and ethnic disparities in Medicare beneficiaries' ability to afford care.
Objective: To examine whether exceeding the income threshold for Medicaid, which results in an abrupt loss of Medicaid eligibility, is associated with greater racial and ethnic disparities in access to and use of care.
Design, setting, and participants: This cross-sectional study used a regression discontinuity design to assess differences in access to and use of care associated with exceeding the income threshold for Medicaid eligibility. We analyzed Medicare beneficiaries with incomes 0% to 200% of FPL from the 2008 to 2018 biennial waves of the Health and Retirement Study linked to Medicare administrative data. To identify racial and ethnic disparities associated with the loss of Medicaid eligibility, we compared discontinuities in outcomes among Black and Hispanic beneficiaries (n = 2885) and White beneficiaries (n = 5259). Analyses were conducted between January 1, 2022, and October 1, 2022.
Main outcome measures: Patient-reported difficulty accessing care due to cost and outpatient service use, medication fills, and hospitalizations measured from Medicare administrative data.
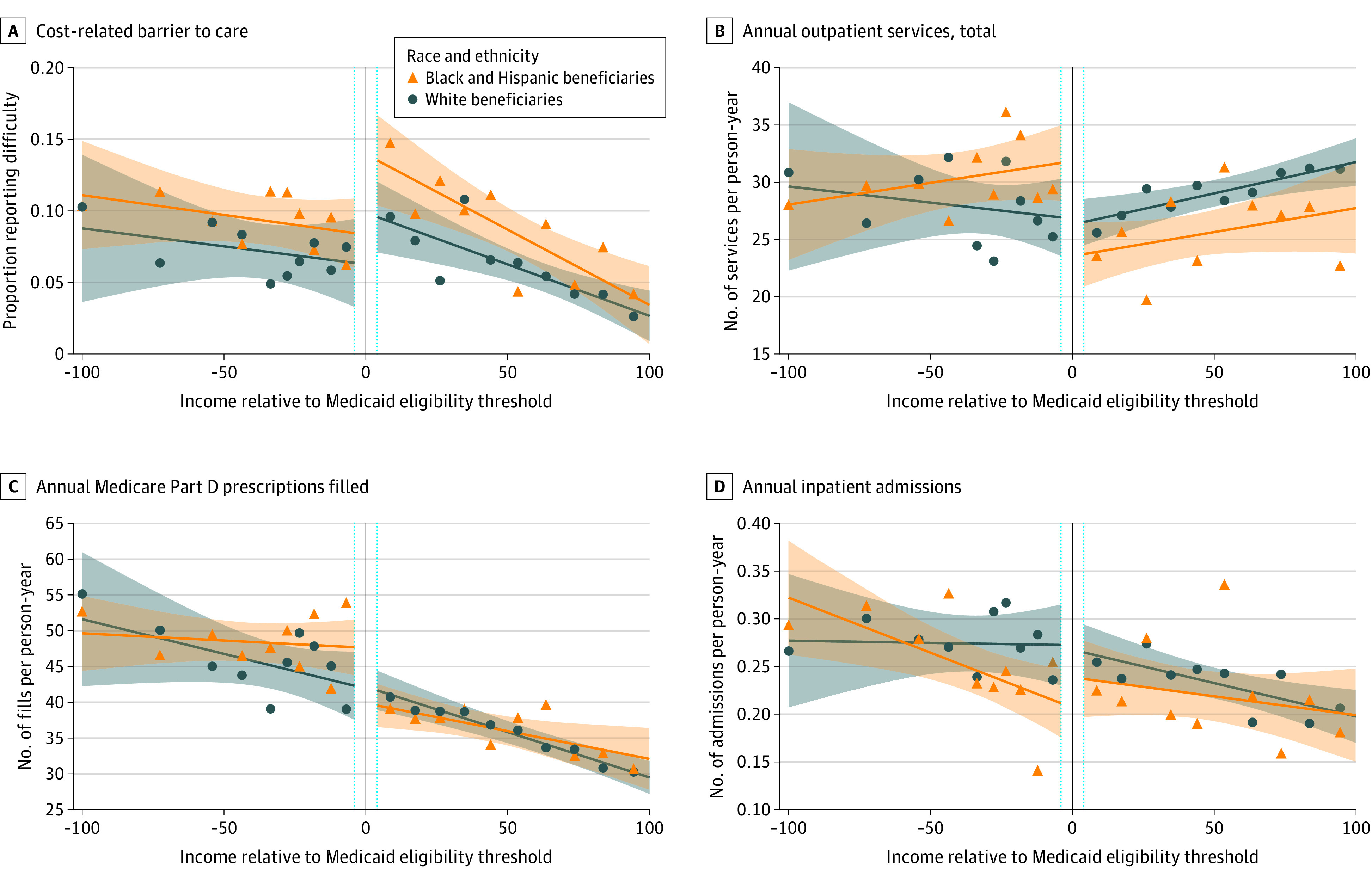
Results: This cross-sectional study included 8144 participants (38 805 person-years), who when weighted represented 151 282 957 person-years in the community-dwelling population of Medicare beneficiaries aged 50 years and older and incomes less than 200% FPL. In the weighted sample, the mean (SD) age was 75.4 (9.4) years, 66.1% of beneficiaries were women, 14.8% were non-Hispanic Black, 13.6% were Hispanic, and 71.6% were White. Findings suggest that exceeding the Medicaid eligibility threshold was associated with a 43.8 percentage point (pp) (95% CI, 37.8-49.8) lower probability of Medicaid enrollment among Black and Hispanic Medicare beneficiaries and a 31.0 pp (95% CI, 25.4-36.6) lower probability of Medicaid enrollment among White beneficiaries. Among Black and Hispanic beneficiaries, exceeding the threshold was associated with increased cost-related barriers to care (discontinuity: 5.7 pp; 95% CI, 2.0-9.4), lower outpatient use (-6.3 services per person-year; 95% CI, -10.4 to -2.2), and fewer medication fills (-6.9 fills per person-year; 95% CI, -11.4 to -2.5), but it was not associated with a statistically significant discontinuity in hospitalizations. Discontinuities in these outcomes were smaller or nonsignificant among White beneficiaries. Consequently, exceeding the threshold was associated with widened disparities, including greater reductions in outpatient service use (disparity: -6.2 services per person-year; 95% CI, -11.7 to -0.6; P = .03) and medication fills (disparity: -7.2 fills per person-year; 95% CI, -13.4 to -1.0; P = .02) among Black and Hispanic vs White beneficiaries.
Conclusions and relevance: This cross-sectional study found that loss of eligibility for Medicaid supplemental insurance above the federal poverty level, which increases cost sharing in Medicare, was associated with increased racial and ethnic health care disparities among low-income Medicare beneficiaries. Expanding eligibility for Medicaid supplemental insurance may narrow these disparities.
Conflict of interest statement
Figures
Comment in
-
Population Weighting in Statistical Analysis.JAMA Intern Med. 2024 Jan 1;184(1):98-99. doi: 10.1001/jamainternmed.2023.6300. JAMA Intern Med. 2024. PMID: 38010717
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
