

Preoperative α-blockade versus no blockade for pheochromocytoma-paraganglioma patients undergoing surgery: a systematic review and updated meta-analysis
- PMID: 37037514
- PMCID: PMC10389437
- DOI: 10.1097/JS9.0000000000000390
Preoperative α-blockade versus no blockade for pheochromocytoma-paraganglioma patients undergoing surgery: a systematic review and updated meta-analysis
Abstract
Background: Surgical resection of pheochromocytomas and paragangliomas (PPGLs) is associated with a significant risk of intraoperative hemodynamic instability and cardiovascular complications. α-blockade remains the routine preoperative medical preparation despite controversies over the lack of evidence. We presented an updated meta-analysis to ulteriorly evaluate the potential efficacy of preoperative α-blockade versus no blockade for PPGL patients undergoing surgery.
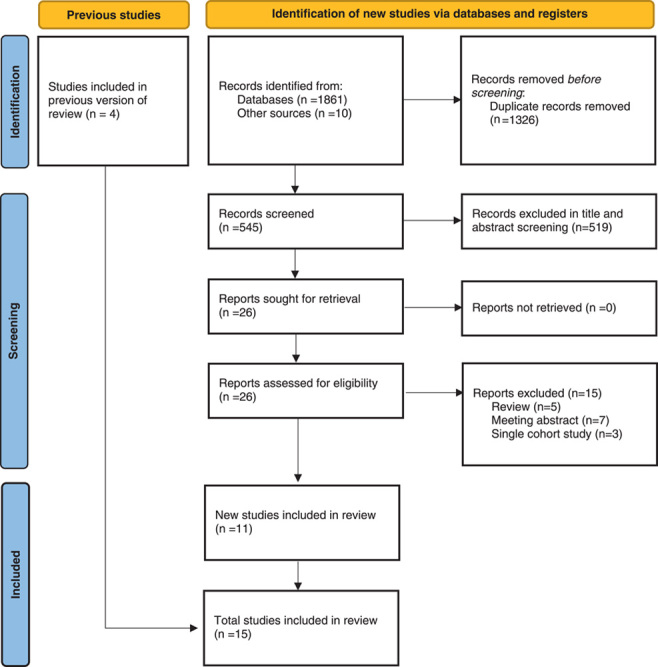
Materials and methods: Randomized and nonrandomized comparative studies assessing preoperative α-blockade for PPGL surgery in adults were identified through a systematic literature search via MEDLINE, Embase, Web of Science, and CENTRAL up to November 2022. Outcome data of intraoperative hemodynamic parameters and major postoperative events were extracted. Mean difference and risk ratio were synthesized as appropriate for each outcome to determine the cumulative effect size.
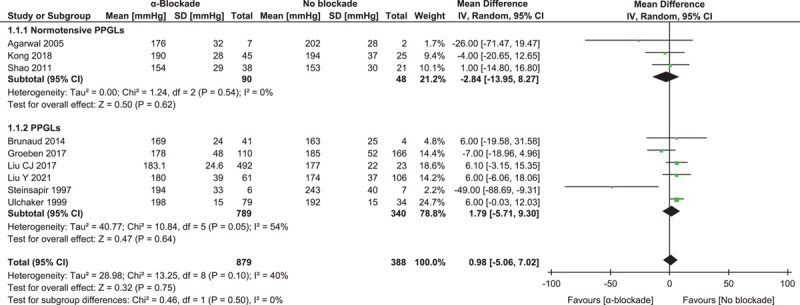
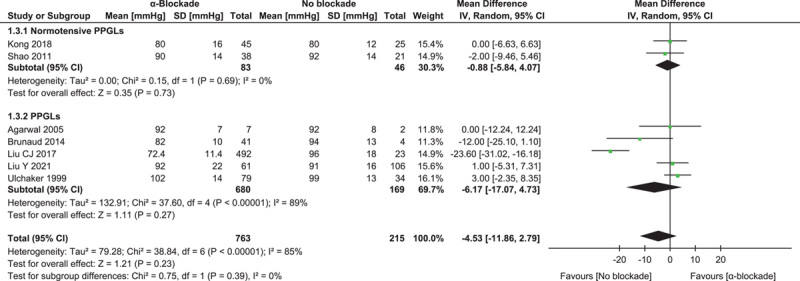
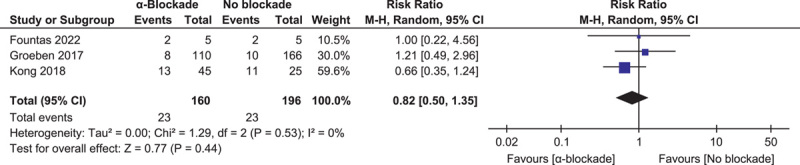
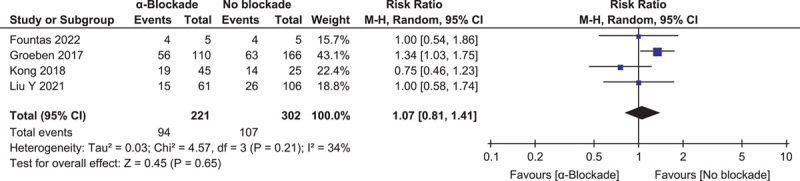
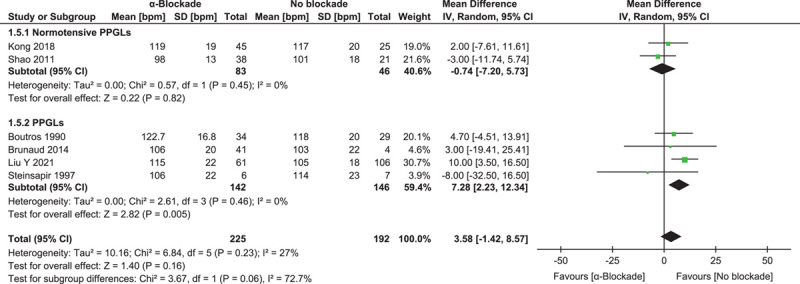
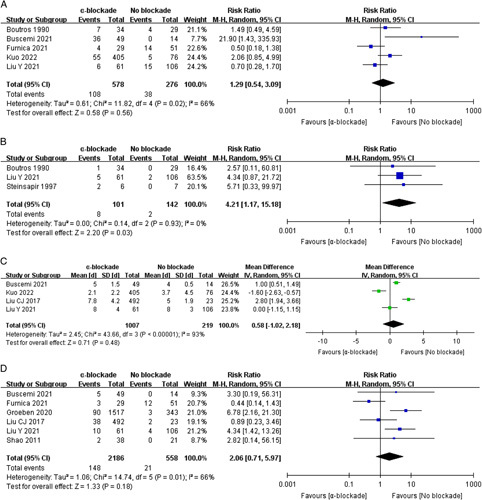
Results: Fifteen nonrandomized studies involving 3542 patients were finally eligible. Intraoperatively, none of the analyzed hemodynamic parameters differed between patients with or without α-blockade: maximum and minimum systolic blood pressure, hypertensive and hypotensive hemodynamic instability episodes, and peak heart rate, subgroup analysis of normotensive PPGL patients yielded similar results with the overall effects. Postoperatively, α-blockade was associated with prolonged hypotension and vasopressor usage (risk ratio: 4.21, 95% CI: 1.17-15.18, P =0.03). ICU admission, length of stay, overall cardiovascular morbidity, and mortality were similar between the two groups.
Conclusions: Preoperative α-blockade ensured neither more stable intraoperative hemodynamics nor better perioperative outcome over no blockade for PPGL surgery. However, large-volume randomized controlled trials are still warranted to ascertain these findings.
Copyright © 2023 The Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors declare that they have no financial conflict of interest with regard to the content of this report.
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.
Figures
Similar articles
-
Preoperative Amlodipine Is Efficacious in Preventing Intraoperative HDI in Pheochromocytoma: Pilot RCT.J Clin Endocrinol Metab. 2021 Jul 13;106(8):e2907-e2918. doi: 10.1210/clinem/dgab231. J Clin Endocrinol Metab. 2021. PMID: 33839787 Clinical Trial.
-
Hemodynamic instability during percutaneous ablation of extra-adrenal metastases of pheochromocytoma and paragangliomas: a case series.BMC Anesthesiol. 2018 Nov 6;18(1):158. doi: 10.1186/s12871-018-0626-1. BMC Anesthesiol. 2018. PMID: 30400849 Free PMC article.
-
Influence of duration of preoperative treatment with phenoxybenzamine and secretory phenotypes on perioperative hemodynamics and postoperative outcomes in pheochromocytoma and paraganglioma.Front Endocrinol (Lausanne). 2023 Apr 19;14:1139015. doi: 10.3389/fendo.2023.1139015. eCollection 2023. Front Endocrinol (Lausanne). 2023. PMID: 37152936 Free PMC article.
-
Selective vs non-selective alpha-blockade prior to adrenalectomy for pheochromocytoma: systematic review and meta-analysis.Eur J Endocrinol. 2021 May 4;184(6):751-760. doi: 10.1530/EJE-20-1301. Eur J Endocrinol. 2021. PMID: 33769959
-
Meta-analysis of α-blockade versus no blockade before adrenalectomy for phaeochromocytoma.Br J Surg. 2020 Jan;107(2):e102-e108. doi: 10.1002/bjs.11348. Br J Surg. 2020. PMID: 31903584
Cited by
-
Short-acting urapidil compared to long-acting phenoxybenzamine in the management of pheochromocytoma.Langenbecks Arch Surg. 2025 Feb 11;410(1):65. doi: 10.1007/s00423-025-03627-6. Langenbecks Arch Surg. 2025. PMID: 39934496 Free PMC article.
-
Pheochromocytoma in MEN2.Recent Results Cancer Res. 2025;223:211-235. doi: 10.1007/978-3-031-80396-3_8. Recent Results Cancer Res. 2025. PMID: 40102259 Review.
-
The expression profiles and roles of microRNAs in cardiac glucose metabolism.Front Endocrinol (Lausanne). 2025 Jul 23;16:1565385. doi: 10.3389/fendo.2025.1565385. eCollection 2025. Front Endocrinol (Lausanne). 2025. PMID: 40771283 Free PMC article.
-
Genetic background and intraoperative haemodynamic instability in patients with pheochromocytoma and paraganglioma: a multicentre retrospective study.Int J Surg. 2025 Jan 1;111(1):913-919. doi: 10.1097/JS9.0000000000001995. Int J Surg. 2025. PMID: 39093877 Free PMC article.
-
Retrospective analysis of robotic versus laparoscopic surgery in the treatment of giant pheochromocytoma and paraganglioma.J Robot Surg. 2025 May 7;19(1):206. doi: 10.1007/s11701-025-02371-9. J Robot Surg. 2025. PMID: 40335861
References
-
- Riester A, Weismann D, Quinkler M, et al. . Life-threatening events in patients with pheochromocytoma. Eur J Endocrinol 2015;173:757–764. - PubMed
-
- Prejbisz A, Lenders JWM, Eisenhofer G, et al. . Cardiovascular manifestations of phaeochromocytoma. J Hypertens 2011;29:2049–2060. - PubMed
-
- Prys-Roberts C. Phaeochromocytoma – recent progress in its management. Br J Anaesth 2000;85:44–57. - PubMed
-
- Lenders JWM, Duh QY, Eisenhofer G, et al. . Pheochromocytoma and paraganglioma: an Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metabol 2014;99:1915–1942. - PubMed
-
- Lenders JWM, Kerstens MN, Amar L, et al. . Genetics, diagnosis, management and future directions of research of phaeochromocytoma and paraganglioma: a position statement and consensus of the Working Group on Endocrine Hypertension of the European Society of Hypertension. J Hypertens 2020;38:1443–1456. - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
