

T cell immune deficiency rather than chromosome instability predisposes patients with short telomere syndromes to squamous cancers
- PMID: 37037617
- PMCID: PMC10188244
- DOI: 10.1016/j.ccell.2023.03.005
T cell immune deficiency rather than chromosome instability predisposes patients with short telomere syndromes to squamous cancers
Abstract
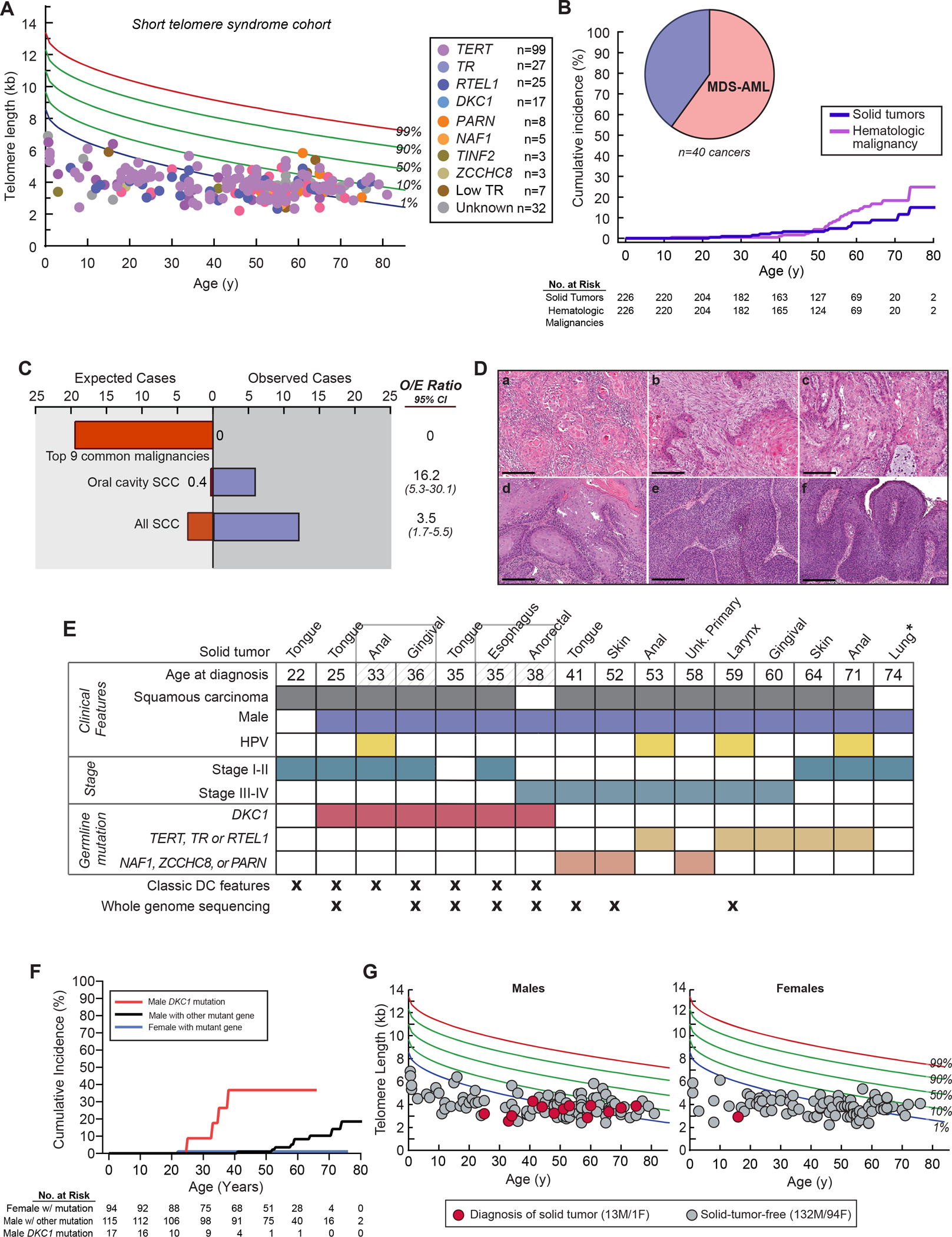
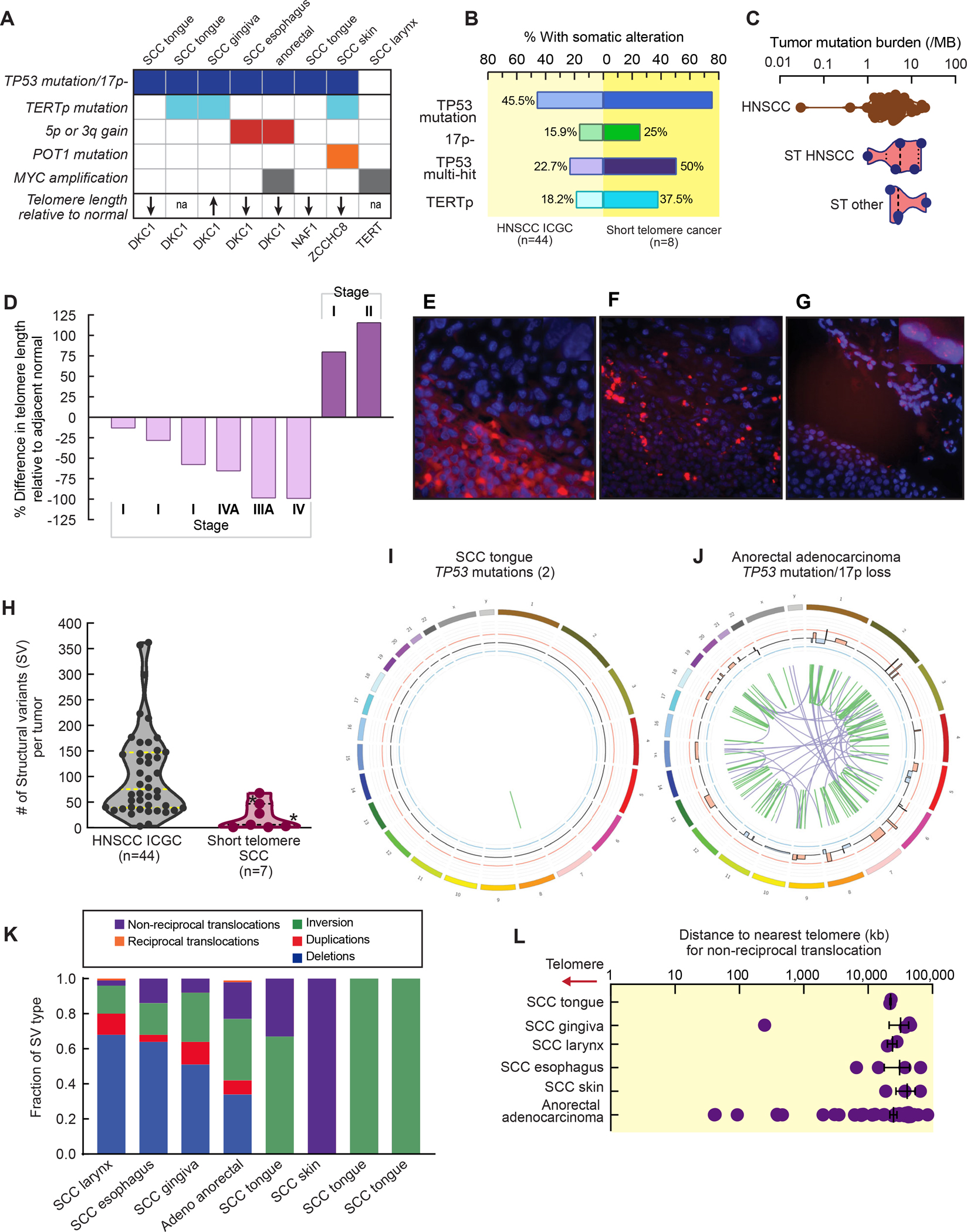
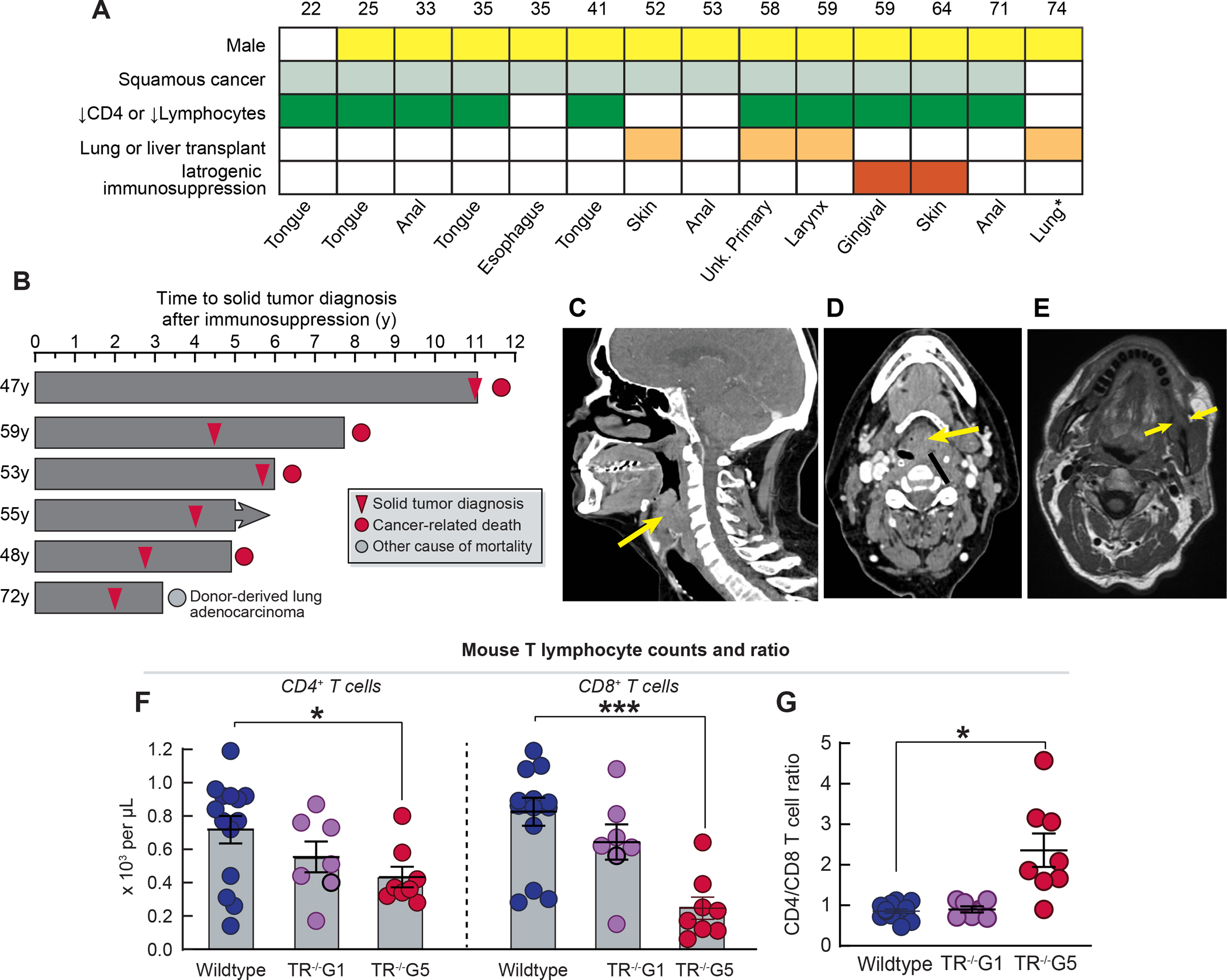
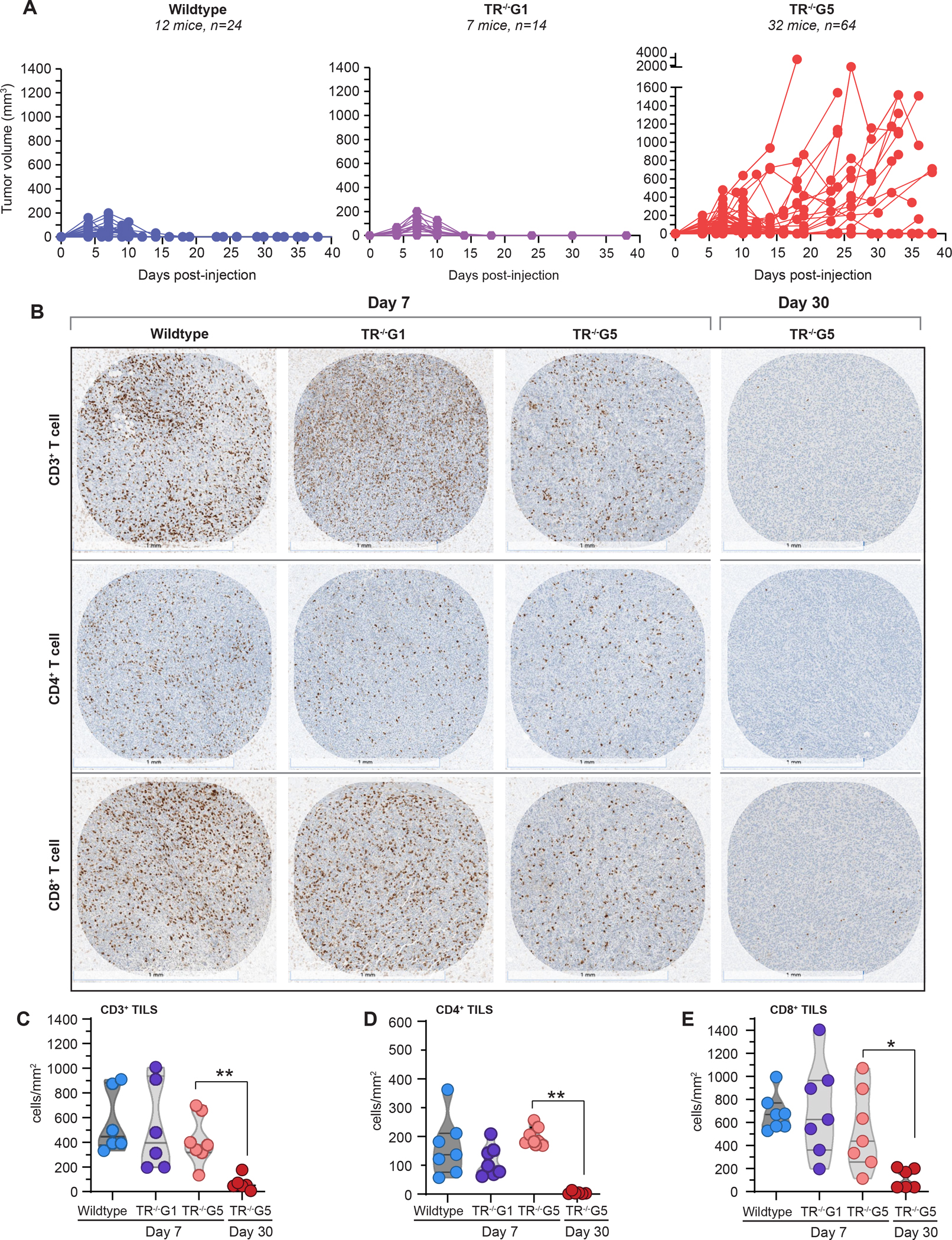
Patients with short telomere syndromes (STS) are predisposed to developing cancer, believed to stem from chromosome instability in neoplastic cells. We tested this hypothesis in a large cohort assembled over the last 20 years. We found that the only solid cancers to which patients with STS are predisposed are squamous cell carcinomas of the head and neck, anus, or skin, a spectrum reminiscent of cancers seen in patients with immunodeficiency. Whole-genome sequencing showed no increase in chromosome instability, such as translocations or chromothripsis. Moreover, STS-associated cancers acquired telomere maintenance mechanisms, including telomerase reverse transcriptase (TERT) promoter mutations. A detailed study of the immune status of patients with STS revealed a striking T cell immunodeficiency at the time of cancer diagnosis. A similar immunodeficiency that impaired tumor surveillance was documented in mice with short telomeres. We conclude that STS patients’ predisposition to solid cancers is due to T cell exhaustion rather than autonomous defects in the neoplastic cells themselves.
Keywords: T cell aging; aging; genome instability; head and neck cancer; immune aging; pulmonary fibrosis; senescence; telomerase.
Copyright © 2023 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of interests R.H.V. is an inventor on licensed patents related to cancer cellular immunotherapy and cancer vaccines, receives royalties from Boston Children’s Hospital for a licensed research-only monoclonal antibody, and has received consulting fees from Bristol Myers Squibb.
Figures
References
-
- Chin L, Artandi SE, Shen Q, Tam A, Lee SL, Gottlieb GJ, Greider CW, and DePinho RA (1999). p53 deficiency rescues the adverse effects of telomere loss and cooperates with telomere dysfunction to accelerate carcinogenesis. Cell 97, 527–538. S0092–8674(00)80762-X [pii]. - PubMed
-
- d’Adda di Fagagna F, Reaper PM, Clay-Farrace L, Fiegler H, Carr P, Von Zglinicki T, Saretzki G, Carter NP, and Jackson SP (2003). A DNA damage checkpoint response in telomere-initiated senescence. Nature 426, 194–198. - PubMed
-
- Lee HW, Blasco MA, Gottlieb GJ, Horner JW 2nd, Greider CW, and DePinho RA (1998). Essential role of mouse telomerase in highly proliferative organs. Nature 392, 569–574. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
