

Cost-effectiveness of pharmaceutical strategies to prevent respiratory syncytial virus disease in young children: a decision-support model for use in low-income and middle-income countries
- PMID: 37038127
- PMCID: PMC10088159
- DOI: 10.1186/s12916-023-02827-5
Cost-effectiveness of pharmaceutical strategies to prevent respiratory syncytial virus disease in young children: a decision-support model for use in low-income and middle-income countries
Abstract
Background: Respiratory syncytial virus (RSV) is a leading cause of respiratory disease in young children. A number of mathematical models have been used to assess the cost-effectiveness of RSV prevention strategies, but these have not been designed for ease of use by multidisciplinary teams working in low-income and middle-income countries (LMICs).
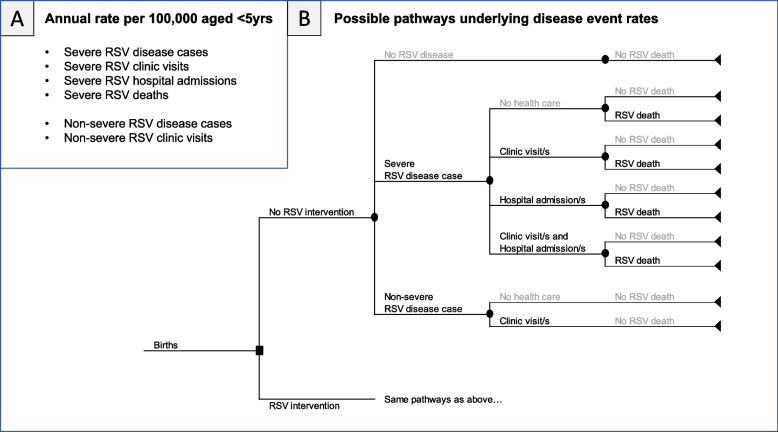
Methods: We describe the UNIVAC decision-support model (a proportionate outcomes static cohort model) and its approach to exploring the potential cost-effectiveness of two RSV prevention strategies: a single-dose maternal vaccine and a single-dose long-lasting monoclonal antibody (mAb) for infants. We identified model input parameters for 133 LMICs using evidence from the literature and selected national datasets. We calculated the potential cost-effectiveness of each RSV prevention strategy (compared to nothing and to each other) over the lifetimes of all children born in the year 2025 and compared our results to a separate model published by PATH. We ran sensitivity and scenario analyses to identify the inputs with the largest influence on the cost-effectiveness results.
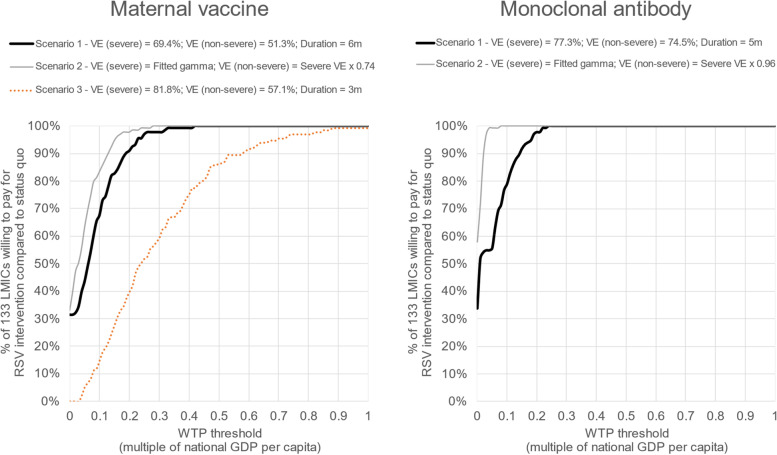
Results: Our illustrative results assuming base case input assumptions for maternal vaccination ($3.50 per dose, 69% efficacy, 6 months protection) and infant mAb ($3.50 per dose, 77% efficacy, 5 months protection) showed that both interventions were cost-saving compared to status quo in around one-third of 133 LMICs, and had a cost per DALY averted below 0.5 times the national GDP per capita in the remaining LMICs. UNIVAC generated similar results to a separate model published by PATH. Cost-effectiveness results were most sensitive to changes in the price, efficacy and duration of protection of each strategy, and the rate (and cost) of RSV hospital admissions.
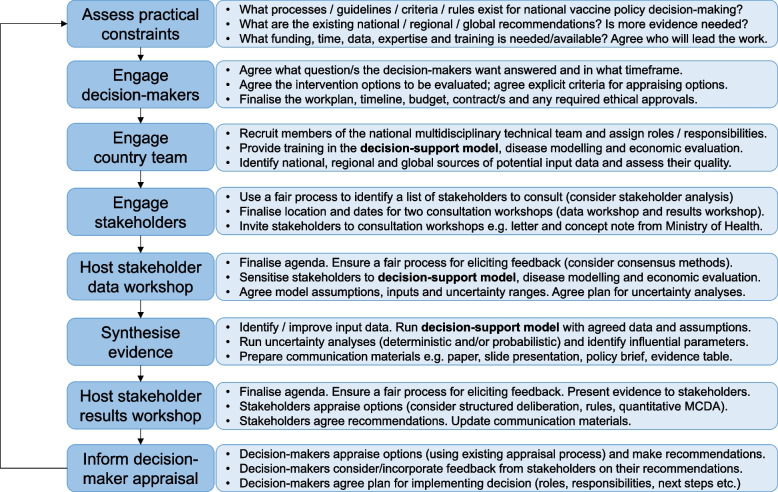
Conclusions: Forthcoming RSV interventions (maternal vaccines and infant mAbs) are worth serious consideration in LMICs, but there is a good deal of uncertainty around several influential inputs, including intervention price, efficacy, and duration of protection. The UNIVAC decision-support model provides a framework for country teams to build consensus on data inputs, explore scenarios, and strengthen the local ownership and policy-relevance of results.
Keywords: Economic evaluation; LMICs; Maternal vaccine; Monoclonal antibody; RSV.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Evaluation of the potential impact and cost-effectiveness of respiratory syncytial virus (RSV) prevention strategies for infants in Argentina.Vaccine. 2024 Oct 3;42(23):126234. doi: 10.1016/j.vaccine.2024.126234. Epub 2024 Aug 17. Vaccine. 2024. PMID: 39154512 Free PMC article.
-
Impact and cost-effectiveness of strategies to prevent respiratory syncytial virus (RSV) disease in Vietnam: A modelling study.Vaccine. 2023 Nov 2;41(46):6782-6790. doi: 10.1016/j.vaccine.2023.09.003. Epub 2023 Sep 9. Vaccine. 2023. PMID: 37690873 Free PMC article.
-
Estimating the cost-effectiveness of maternal vaccination and monoclonal antibodies for respiratory syncytial virus in Kenya and South Africa.BMC Med. 2023 Mar 31;21(1):120. doi: 10.1186/s12916-023-02806-w. BMC Med. 2023. PMID: 37004062 Free PMC article.
-
Cost of childhood RSV management and cost-effectiveness of RSV interventions: a systematic review from a low- and middle-income country perspective.BMC Med. 2023 Mar 31;21(1):121. doi: 10.1186/s12916-023-02792-z. BMC Med. 2023. PMID: 37004038 Free PMC article.
-
Assessment of the Effects of Active Immunisation against Respiratory Syncytial Virus (RSV) using Decision-Analytic Models: A Systematic Review with a Focus on Vaccination Strategies, Modelling Methods and Input Data.Pharmacoeconomics. 2021 Mar;39(3):287-315. doi: 10.1007/s40273-020-00991-7. Epub 2021 Jan 19. Pharmacoeconomics. 2021. PMID: 33462760 Free PMC article.
Cited by
-
Characteristics of inpatient and outpatient respiratory syncytial virus mortality in Gavi-eligible countries.Vaccine X. 2024 Sep 13;20:100554. doi: 10.1016/j.jvacx.2024.100554. eCollection 2024 Oct. Vaccine X. 2024. PMID: 39315335 Free PMC article.
-
Trends in the Mortality, Deaths, and Aetiologies of Lower Respiratory Infections Among 204 Countries from 1991 to 2021: An Updated Systematic Study.Viruses. 2025 Jun 25;17(7):892. doi: 10.3390/v17070892. Viruses. 2025. PMID: 40733510 Free PMC article.
-
What will it take? Perspectives from five low- and middle-income countries on opportunities and challenges of introducing new maternal vaccines.Vaccine. 2025 Jan 25;45:126654. doi: 10.1016/j.vaccine.2024.126654. Epub 2024 Dec 24. Vaccine. 2025. PMID: 39721352 Free PMC article.
-
Incidence of Respiratory Syncytial Virus-Associated Lower Respiratory Tract Infection Until 6 months of Corrected Age in Preterm Infants with Bronchopulmonary Dysplasia: A Pilot Prospective Cohort Study.Indian J Pediatr. 2025 Jun 5. doi: 10.1007/s12098-025-05577-9. Online ahead of print. Indian J Pediatr. 2025. PMID: 40471395
-
Cost-effectiveness analysis of the 13-valent pneumococcal conjugate vaccine administered to children under 5 years of age in the Republic of Moldova.Med Pharm Rep. 2025 Jan;98(1):111-117. doi: 10.15386/mpr-2674. Epub 2025 Jan 31. Med Pharm Rep. 2025. PMID: 39949911 Free PMC article.
References
-
- Li Y, Wang X, Blau DM, Caballero MT, Feikin DR, Gill CJ, et al. Global, regional, and national disease burden estimates of acute lower respiratory infections due to respiratory syncytial virus in children younger than 5 years in 2019: a systematic analysis. Lancet. 2022;399(10340):2047–2064. doi: 10.1016/S0140-6736(22)00478-0. - DOI - PMC - PubMed
-
- IMpact-RSV Study Group. Palivizumab, a humanized respiratory syncytial virus monoclonal antibody, reduces hospitalization from respiratory syncytial virus infection in high-risk infants. Pediatrics. 1998;102(3):531–7. - PubMed
-
- AstraZeneca. Medicines. [Available from: https://www.astrazeneca.co.uk/medicines-AZ.html#. Accessed 15 Dec 2021.
-
- American Academy of Pediatrics Committee on Infectious Diseases; American Academy of Pediatrics Bronchiolitis Guidelines Committee. Updated guidance for palivizumab prophylaxis among infants and young children at increased risk of hospitalization for respiratory syncytial virus infection. Pediatrics. 2014;134(2):e620–38. - PubMed
-
- Teale A, Deshpande S, Burls A. Palivizumab and the importance of cost effectiveness. BMJ. 2009;338:b1935.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
