

Operative Hysteroscopy vs Vacuum Aspiration for Incomplete Spontaneous Abortion: A Randomized Clinical Trial
- PMID: 37039805
- PMCID: PMC10091175
- DOI: 10.1001/jama.2023.3415
Operative Hysteroscopy vs Vacuum Aspiration for Incomplete Spontaneous Abortion: A Randomized Clinical Trial
Erratum in
-
Incorrect Interquartile Ranges.JAMA. 2023 Sep 26;330(12):1194. doi: 10.1001/jama.2023.17492. JAMA. 2023. PMID: 37750889 Free PMC article. No abstract available.
Abstract
Importance: Vacuum aspiration is commonly used to remove retained products of conception in patients with incomplete spontaneous abortion. Scarring of the uterine cavity may occur, potentially impairing future fertility. A procedural alternative, operative hysteroscopy, has gained popularity with a presumption of better future fertility.
Objective: To assess the superiority of hysteroscopy to vacuum aspiration for subsequent pregnancy in patients with incomplete spontaneous abortion who intend to have future pregnancy.
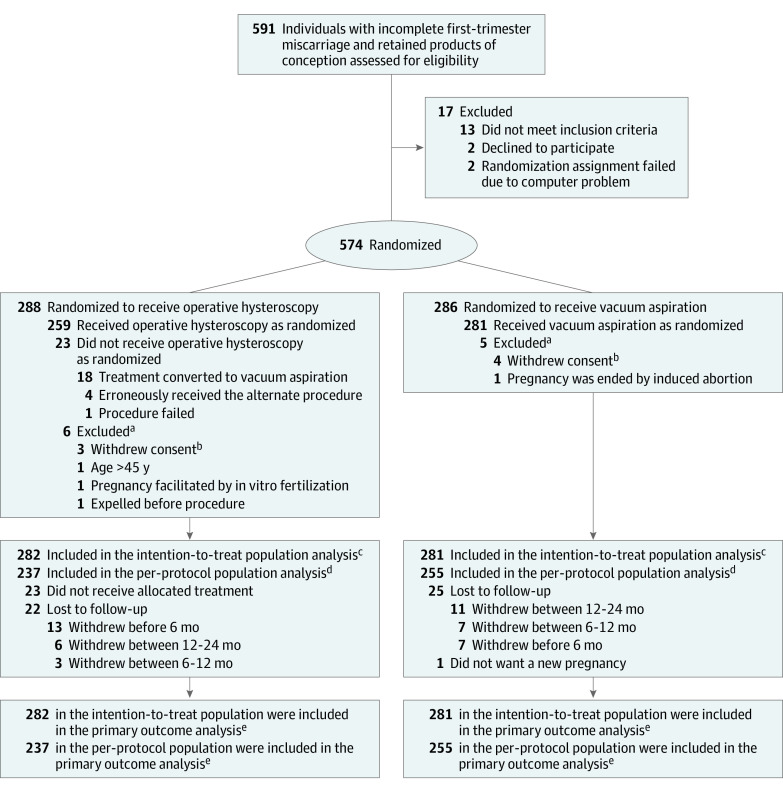
Design, setting, and participants: The HY-PER randomized, controlled, single-blind trial included 574 patients between November 6, 2014, and May 3, 2017, with a 2-year duration of follow-up. This multicenter trial recruited patients in 15 French hospitals. Individuals aged 18 to 44 years and planned for surgery for an incomplete spontaneous abortion with plans to subsequently conceive were randomized in a 1:1 ratio.
Interventions: Surgical treatment by hysteroscopy (n = 288) or vacuum aspiration (n = 286).
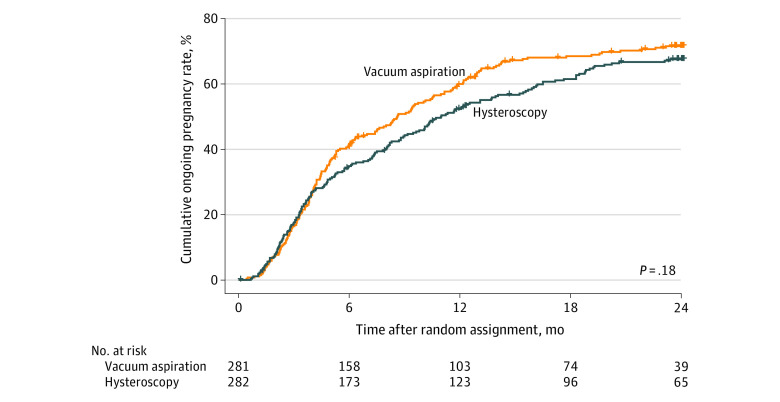
Main outcomes and measures: The primary outcome was a pregnancy of at least 22 weeks' duration during 2-year follow-up.
Results: The intention-to-treat analyses included 563 women (mean [SD] age, 32.6 [5.4] years). All aspiration procedures were completed. The hysteroscopic procedure could not be completed for 19 patients (7%), 18 of which were converted to vacuum aspiration (8 with inability to completely resect, 7 with insufficient visualization, 2 with anesthetic complications that required a shortened procedure, 1 with equipment failure). One hysteroscopy failed due to a false passage during cervical dilatation. During the 2-year follow-up, 177 patients (62.8%) in the hysteroscopy group and 190 (67.6%) in the vacuum aspiration (control) group achieved the primary outcome (difference, -4.8% [95% CI, -13% to 3.0%]; P = .23). The time-to-event analyses showed no statistically significant difference between groups for the primary outcome (hazard ratio, 0.87 [95% CI, 0.71 to 1.07]). Duration of surgery and hospitalization were significantly longer for hysteroscopy. Rates of new miscarriages, ectopic pregnancies, Clavien-Dindo surgical complications of grade 3 or above (requiring surgical, endoscopic, or radiological intervention or life-threatening event or death), and reinterventions to remove remaining products of conception did not differ between groups.
Conclusions and relevance: Surgical management by hysteroscopy of incomplete spontaneous abortions in patients intending to conceive again was not associated with more subsequent births or a better safety profile than vacuum aspiration. Moreover, operative hysteroscopy was not feasible in all cases.
Trial registration: ClinicalTrials.gov Identifier: NCT02201732.
Conflict of interest statement
Figures
Comment in
-
Variations in Care for Early Pregnancy Loss Across Clinical Settings.JAMA Netw Open. 2023 Mar 1;6(3):e232645. doi: 10.1001/jamanetworkopen.2023.2645. JAMA Netw Open. 2023. PMID: 36920399 No abstract available.
-
Excerpts from World Medical Literature: Gynaecology.J Obstet Gynaecol Can. 2023 Dec;45(12):102247. doi: 10.1016/j.jogc.2023.102247. J Obstet Gynaecol Can. 2023. PMID: 38049283 No abstract available.
-
Extraits de la littérature médicale mondiale : Gynécologie.J Obstet Gynaecol Can. 2023 Dec;45(12):102296. doi: 10.1016/j.jogc.2023.102296. J Obstet Gynaecol Can. 2023. PMID: 38049284 No abstract available.
