

VA's implementation of universal screening and evaluation for the suicide risk identification program in November 2020 -Implications for Veterans with prior mental health needs
- PMID: 37040367
- PMCID: PMC10089346
- DOI: 10.1371/journal.pone.0283633
VA's implementation of universal screening and evaluation for the suicide risk identification program in November 2020 -Implications for Veterans with prior mental health needs
Abstract
Importance: United States Veterans are at higher risk for suicide than non-Veterans. Veterans in rural areas are at higher risk than their urban counterparts. The coronavirus pandemic intensified risk factors for suicide, especially in rural areas.
Objective: To examine associations between Veterans Health Administration's (VA's) universal suicide risk screening, implemented November 2020, and likelihood of Veterans being screened, and receiving follow-up evaluations, as well as post-screening suicidal behavior among patients who used VA mental health services in 2019.
Methods: VA's Suicide Risk Identification Strategy (Risk ID), implemented October 2018, is a national, standardized process for suicide risk screening and evaluation. In November 2020, VA expanded Risk ID, requiring annual universal suicide screening. As such, we are evaluating outcomes of interest before and after the start of the policy among Veterans who had ≥1 VA mental health care visit in 2019 (n = 1,654,180; rural n = 485,592, urban n = 1,168,588). Regression-adjusted outcomes were compared 6 months pre-universal screening and 6, 12 and 13 months post-universal screening implementation.
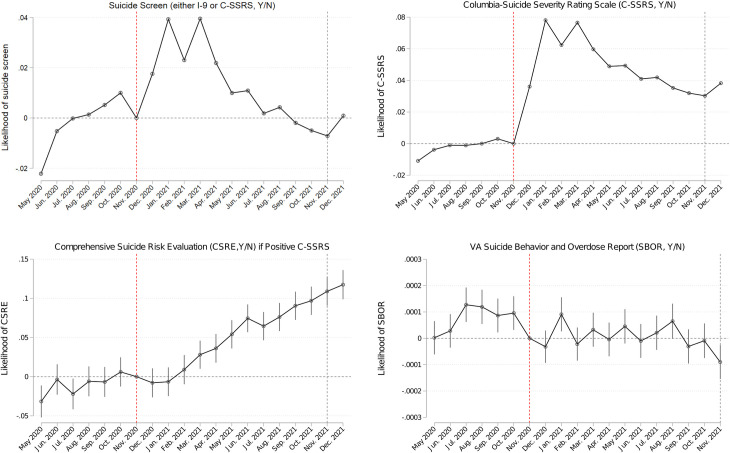
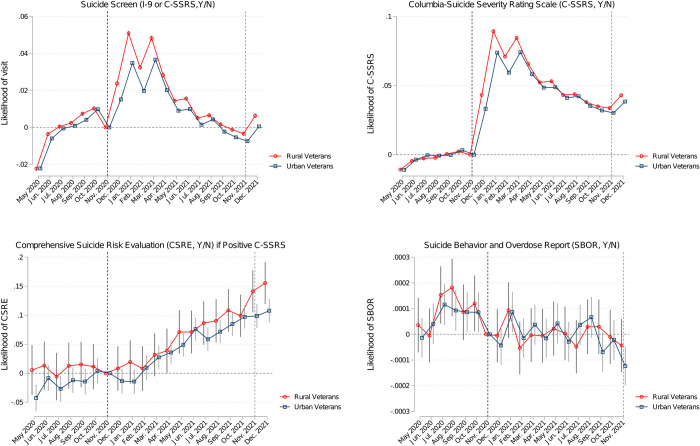
Measures: Item-9 on the Patient Health Questionnaire (I-9, VA's historic suicide screener), Columbia- Suicide Severity Risk Scale (C-SSRS) Screener, VA's Comprehensive Suicide Risk Evaluation (CSRE), and Suicide Behavior and Overdose Report (SBOR).
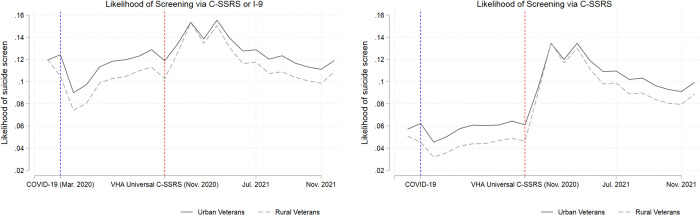
Results: 12 months post-universal screening implementation, 1.3 million Veterans (80% of the study cohort) were screened or evaluated for suicide risk, with 91% the sub-cohort who had at least one mental health visit in the 12 months post-universal screening implementation period were screened or evaluated. At least 20% of the study cohort was screened outside of mental health care settings. Among Veterans with positive screens, 80% received follow-up CSREs. Covariate-adjusted models indicated that an additional 89,160 Veterans were screened per month via the C-SSRS and an additional 30,106 Veterans/month screened via either C-SSRS or I-9 post-universal screening implementation. Compared to their urban counterparts, 7,720 additional rural Veterans/month were screened via the C-SSRS and 9,226 additional rural Veterans/month were screened via either the C-SSRS or I-9.
Conclusion: VA's universal screening requirement via VA's Risk ID program increased screening for suicide risk among Veterans with mental health care needs. A universal approach to screening may be particularly advantageous for rural Veterans, who are typically at higher risk for suicide but have fewer interactions with the health care system, particularly within specialty care settings, due to higher barriers to accessing care. Insights from this program offer valuable insights for health systems nationwide.
Copyright: This is an open access article, free of all copyright, and may be freely reproduced, distributed, transmitted, modified, built upon, or otherwise used by anyone for any lawful purpose. The work is made available under the Creative Commons CC0 public domain dedication.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Office of Mental Health and Suicide Prevention. 2021 National Veteran Suicide Prevention Annual Report. US Department of Veterans Affairs. 2021. Available: https://www.mentalhealth.va.gov/docs/data-sheets/2021/2021-National-Vete....
-
- The Joint Commission. R3 Report: Requirement, Rationale, Reference. 2019. Available: https://www.jointcommission.org/-/media/tjc/documents/standards/r3-repor....
-
- Office of Mental Health and Suicide Prevention. 2019 National Veteran Suicide Prevention Annual Report. US Department of Veterans Affairs. 2019. Available: https://www.mentalhealth.va.gov/docs/data-sheets/2019/2019_National_Vete....
-
- U.S. Department of Veterans Affairs. National Veteran Suicide Prevention Annual Report. 2020. Available: https://www.mentalhealth.va.gov/docs/data-sheets/2020/2020-National-Vete....
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
