

Evidence for key individual characteristics associated with outcomes following combined first-line interventions for knee osteoarthritis: A systematic review
- PMID: 37040393
- PMCID: PMC10089365
- DOI: 10.1371/journal.pone.0284249
Evidence for key individual characteristics associated with outcomes following combined first-line interventions for knee osteoarthritis: A systematic review
Abstract
Objective: To identify individual characteristics associated with outcomes following combined first-line interventions for knee osteoarthritis.
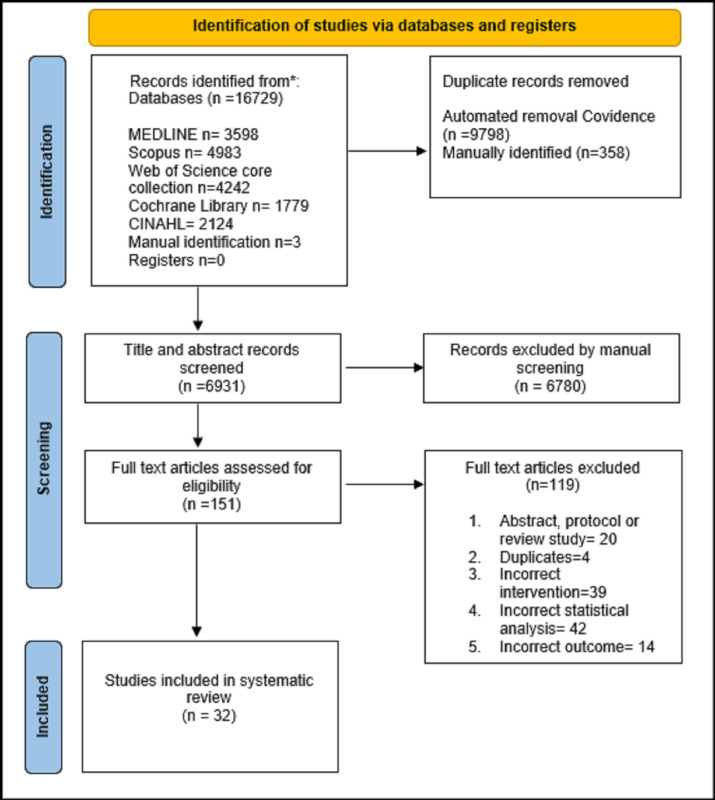
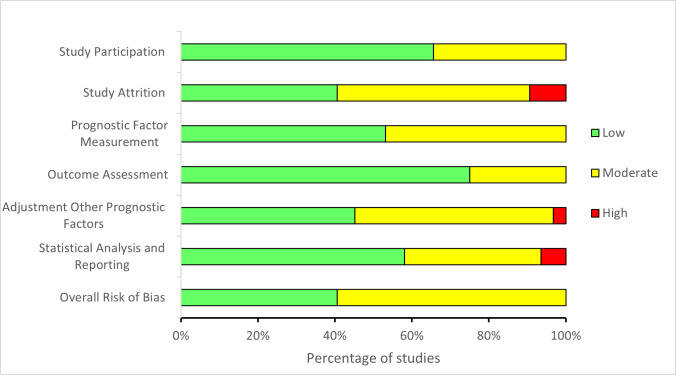
Methods: MEDLINE, CINAHL, Scopus, Web of Science Core Collection and the Cochrane library were searched. Studies were included if they reported an association between baseline factors and change in pain or function following combined exercise therapy, osteoarthritis education, or weight management interventions for knee osteoarthritis. Risk of bias was assessed using Quality in Prognostic Factor Studies. Data was visualised and a narrative synthesis was conducted for key factors (age, sex, BMI, comorbidity, depression, and imaging severity).
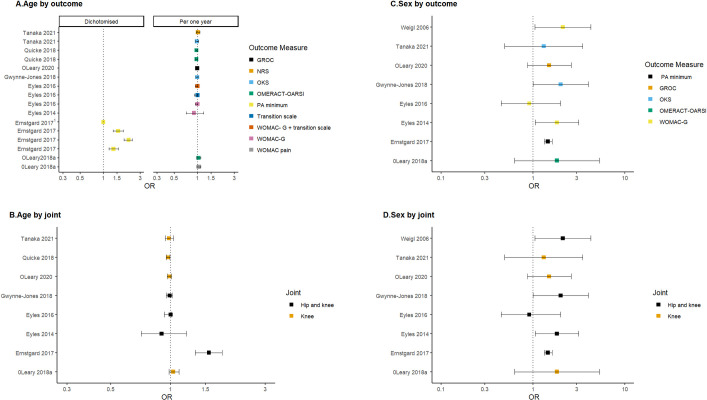
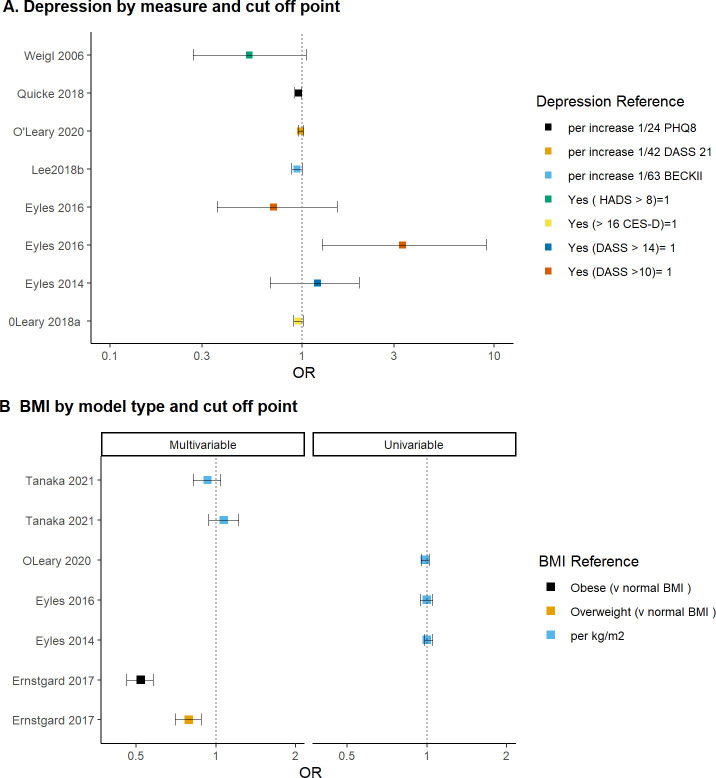
Results: 32 studies were included. Being female compared to male was associated with 2-3 times the odds of a positive response. Older age was associated with reduced odds of a positive response. The effect size (less than 10% reduction) is unlikely to be clinically relevant. It was difficult to conclude whether BMI, comorbidity, depression and imaging severity were associated with pain and function outcomes following a combined first-line intervention for knee osteoarthritis. Low to very low certainty evidence was found for sex, BMI, depression, comorbidity and imaging severity and moderate certainty evidence for age. Varying study methods contributed to some difficulty in drawing clear conclusions.
Conclusions: This systematic review found no clear evidence to suggest factors such as age, sex, BMI, OA severity and presence of depression or comorbidities are associated with the response to first-line interventions for knee OA. Current evidence indicates that some groups of people may respond equally to first-line interventions, such as those with or without comorbidities. First-line interventions consisting of exercise therapy, education, and weight loss for people with knee OA should be recommended irrespective of sex, age, obesity, comorbidity, depression and imaging findings.
Copyright: © 2023 Couldrick et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Factors Associated With the Outcome of a First-Line Intervention for Patients With Hip or Knee Osteoarthritis or Both: Data From the BOA Register.Phys Ther. 2020 Sep 28;100(10):1771-1781. doi: 10.1093/ptj/pzaa113. Phys Ther. 2020. PMID: 32589713 Free PMC article.
-
Do comorbidities predict pain and function in knee osteoarthritis following an exercise intervention, and do they moderate the effect of exercise? Analyses of data from three randomized controlled trials.Musculoskeletal Care. 2020 Mar;18(1):3-11. doi: 10.1002/msc.1425. Epub 2019 Dec 14. Musculoskeletal Care. 2020. PMID: 31837126 Clinical Trial.
-
Development of comorbidity-adapted exercise protocols for patients with knee osteoarthritis.Clin Interv Aging. 2014 May 14;9:829-42. doi: 10.2147/CIA.S55705. eCollection 2014. Clin Interv Aging. 2014. PMID: 24868151 Free PMC article. Clinical Trial.
-
The Efficacy of Electronic Health-Supported Home Exercise Interventions for Patients With Osteoarthritis of the Knee: Systematic Review.J Med Internet Res. 2018 Apr 26;20(4):e152. doi: 10.2196/jmir.9465. J Med Internet Res. 2018. PMID: 29699963 Free PMC article.
-
Patient education improves pain and function in people with knee osteoarthritis with better effects when combined with exercise therapy: a systematic review.J Physiother. 2021 Jul;67(3):177-189. doi: 10.1016/j.jphys.2021.06.011. Epub 2021 Jun 20. J Physiother. 2021. PMID: 34158270
Cited by
-
Pro-Inflammatory Biomarkers Combined with Body Composition Display a Strong Association with Knee Osteoarthritis in a Community-Based Study.Biomolecules. 2023 Aug 28;13(9):1315. doi: 10.3390/biom13091315. Biomolecules. 2023. PMID: 37759715 Free PMC article.
-
Reconsidering the Role of Weight Loss in Treatment for Chronic Pain: Knee Osteoarthritis as an Exemplar.J Pain. 2024 Dec;25(12):104647. doi: 10.1016/j.jpain.2024.104647. Epub 2024 Aug 3. J Pain. 2024. PMID: 39103008 Review.
-
Adipose- and bone marrow-derived stromal cells reduce pain in patients with knee osteoarthritis but do not substantially improve knee functionality: an updated systematic review and meta-analysis.Eur J Orthop Surg Traumatol. 2025 May 23;35(1):214. doi: 10.1007/s00590-025-04322-4. Eur J Orthop Surg Traumatol. 2025. PMID: 40407910 Free PMC article. Review.
-
Osteoarthritis.Nat Rev Dis Primers. 2025 Feb 13;11(1):10. doi: 10.1038/s41572-025-00594-6. Nat Rev Dis Primers. 2025. PMID: 39948092 Review.
-
Five-Year Impact of Weight Loss on Knee Pain and Quality of Life in Obese Patients.Med Sci Monit. 2025 Jan 20;31:e946550. doi: 10.12659/MSM.946550. Med Sci Monit. 2025. PMID: 39829029 Free PMC article.
References
-
- Bennell KL, Bayram C, Harrison C, Brand C, Buchbinder R, Haas R, et al.. Trends in management of hip and knee osteoarthritis in general practice in Australia over an 11-year window: a nationwide cross-sectional survey. Lancet Reg Health West Pac. 2021;12:100187. Epub 20210609. doi: 10.1016/j.lanwpc.2021.100187 ; PubMed Central PMCID: PMC8356093. - DOI - PMC - PubMed
-
- Eyles JP, Hunter DJ, Bennell KL, Dziedzic KS, Hinman RS, van der Esch M, et al.. Priorities for the effective implementation of osteoarthritis management programs: an OARSI international consensus exercise. Osteoarthritis and Cartilage. 2019;27(9):1270–9. doi: 10.1016/j.joca.2019.05.015 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
