

The return of the lesion for localization and therapy
- PMID: 37040563
- PMCID: PMC10393408
- DOI: 10.1093/brain/awad123
The return of the lesion for localization and therapy
Abstract
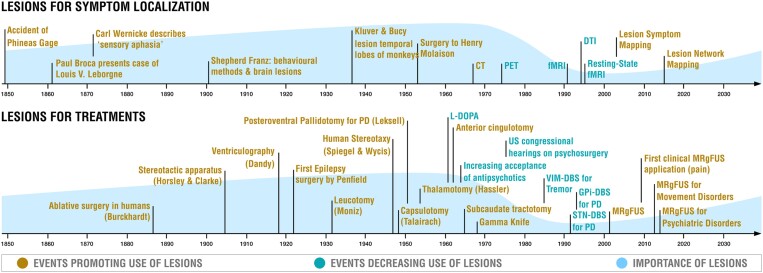
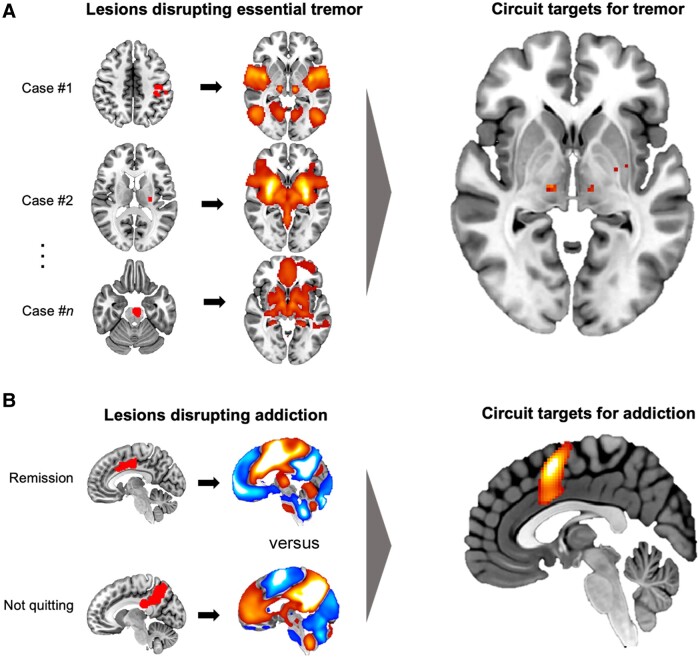
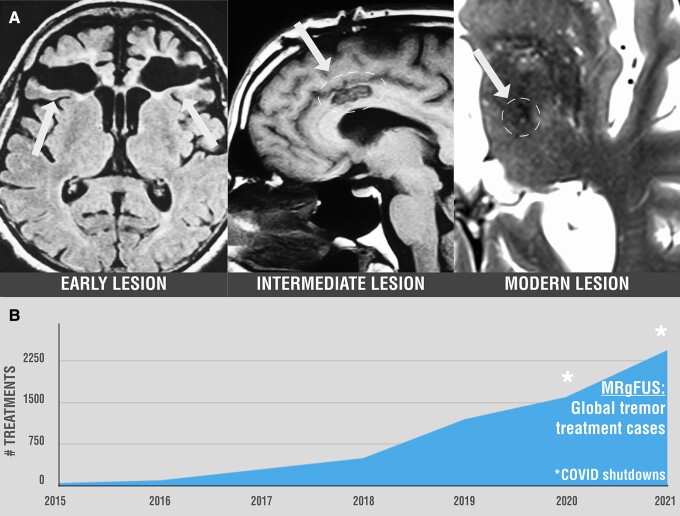
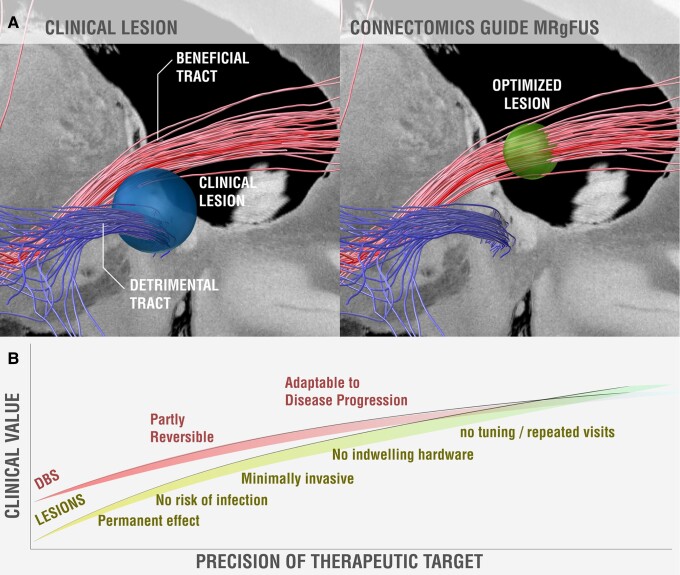
Historically, pathological brain lesions provided the foundation for localization of symptoms and therapeutic lesions were used as a treatment for brain diseases. New medications, functional neuroimaging and deep brain stimulation have led to a decline in lesions in the past few decades. However, recent advances have improved our ability to localize lesion-induced symptoms, including localization to brain circuits rather than individual brain regions. Improved localization can lead to more precise treatment targets, which may mitigate traditional advantages of deep brain stimulation over lesions such as reversibility and tunability. New tools for creating therapeutic brain lesions such as high intensity focused ultrasound allow for lesions to be placed without a skin incision and are already in clinical use for tremor. Although there are limitations, and caution is warranted, improvements in lesion-based localization are refining our therapeutic targets and improved technology is providing new ways to create therapeutic lesions, which together may facilitate the return of the lesion.
Keywords: MRgFUS; connectivity; lesion mapping; lesion network mapping; stroke.
© The Author(s) 2023. Published by Oxford University Press on behalf of the Guarantors of Brain.
Conflict of interest statement
J.J. has received conference travel support from Abbvie and Abbott and lecturer honoraria from Lundbeck and Novartis. N.L. reports grants from Weston Brain Institute Focused Ultrasound Foundation and serves as an expert in the Steering Committee by Focused Ultrasound Foundation. A.H. reports lecture fees from Boston Scientific unrelated to the present work. G.R.C. is a consultant for Insightec Inc. and Clearpoint Neuro Inc. M.D.F. is a consultant for Magnus Medical, Soterix and Boston Scientific, and has one existing and one submitted patent on using brain connectivity to find targets for brain stimulation–no royalties.
Figures
Similar articles
-
Network localization of neurological symptoms from focal brain lesions.Brain. 2015 Oct;138(Pt 10):3061-75. doi: 10.1093/brain/awv228. Epub 2015 Aug 10. Brain. 2015. PMID: 26264514 Free PMC article.
-
Lesion network mapping for symptom localization: recent developments and future directions.Curr Opin Neurol. 2022 Aug 1;35(4):453-459. doi: 10.1097/WCO.0000000000001085. Epub 2022 Jul 5. Curr Opin Neurol. 2022. PMID: 35788098 Free PMC article. Review.
-
The potential value of probabilistic tractography-based for MR-guided focused ultrasound thalamotomy for essential tremor.Neuroimage Clin. 2017 Dec 12;17:1019-1027. doi: 10.1016/j.nicl.2017.12.018. eCollection 2018. Neuroimage Clin. 2017. PMID: 29527503 Free PMC article.
-
Lesion network localization of free will.Proc Natl Acad Sci U S A. 2018 Oct 16;115(42):10792-10797. doi: 10.1073/pnas.1814117115. Epub 2018 Oct 1. Proc Natl Acad Sci U S A. 2018. PMID: 30275309 Free PMC article.
-
Lesion voxels to lesion networks: The enduring value of the Vietnam Head Injury Study.Cortex. 2024 Mar;172:109-113. doi: 10.1016/j.cortex.2023.12.006. Epub 2023 Dec 30. Cortex. 2024. PMID: 38271817 Review.
Cited by
-
Sensing, feeling and regulating: investigating the association of focal brain damage with voluntary respiratory and motor control.Philos Trans R Soc Lond B Biol Sci. 2024 Aug 26;379(1908):20230251. doi: 10.1098/rstb.2023.0251. Epub 2024 Jul 15. Philos Trans R Soc Lond B Biol Sci. 2024. PMID: 39005040 Free PMC article.
-
Bilateral Focused Ultrasound Thalamotomy for Essential Tremor: Clinical Outcomes Compared to Bilateral Deep Brain Stimulation and Probabilistic Lesion Mapping.Mov Disord. 2025 Jul;40(7):1265-1278. doi: 10.1002/mds.30221. Epub 2025 May 2. Mov Disord. 2025. PMID: 40318052 Free PMC article.
-
Multimodal neuroimaging to characterize symptom-specific networks in movement disorders.NPJ Parkinsons Dis. 2024 Aug 14;10(1):154. doi: 10.1038/s41531-024-00774-3. NPJ Parkinsons Dis. 2024. PMID: 39143114 Free PMC article. Review.
-
Functional anatomy of the subthalamic nucleus and the pathophysiology of cardinal features of Parkinson's disease unraveled by focused ultrasound ablation.Sci Adv. 2024 Nov 22;10(47):eadr9891. doi: 10.1126/sciadv.adr9891. Epub 2024 Nov 22. Sci Adv. 2024. PMID: 39576853 Free PMC article.
-
Convergent mapping of a tremor treatment network.Nat Commun. 2025 May 22;16(1):4772. doi: 10.1038/s41467-025-60089-6. Nat Commun. 2025. PMID: 40404653 Free PMC article.
References
-
- Blomstedt P, Hariz MI. Deep brain stimulation for movement disorders before DBS for movement disorders. Parkinsonism Relat Disord. 2010;16:429–433. - PubMed
-
- Hariz MI, Blomstedt P, Zrinzo L. Deep brain stimulation between 1947 and 1987: the untold story. Neurosurg Focus. 2010;29:E1. - PubMed
-
- Bergman H, Wichmann T, DeLong MR. Reversal of experimental parkinsonism by lesions of the subthalamic nucleus. Science. 1990;249:1436–1438. - PubMed
-
- Goodale MA, Milner AD, Jakobson LS, Carey DP. A neurological dissociation between perceiving objects and grasping them. Nature. 1991;349:154–156. - PubMed
-
- Damasio H, Damasio A. Lesion analysis in neuropsychology: Oxford University Press; 1989.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
